
June 2015
It is hard not to right an essay when it comes to thyroid scanning. Thyroids can bedevil us all and no rule is absolute when it comes to thyroid nodules. For a more in depth discussion about which nodules need biopsy see here. Nevertheless here are a few common pitfalls.
Not everything abnormal in the thyroid is a nodule. If there is no normal thyroid tissue present it almost certainly is a thyroiditis (put the colour on). Thyroiditis can be vary patchy and both the affected and the unaffected areas can appear as nodular. If there is no normal tissue and the only “nodules” present are small and echogenic then ask yourself “Could these be islands of normal thyroid tissue” or pseudo-nodules? If they are tiny and hypoechoic they may be lymphoctic aggregates typical of Hashimoto’s (or sometimes Graves’ thyroiditis).
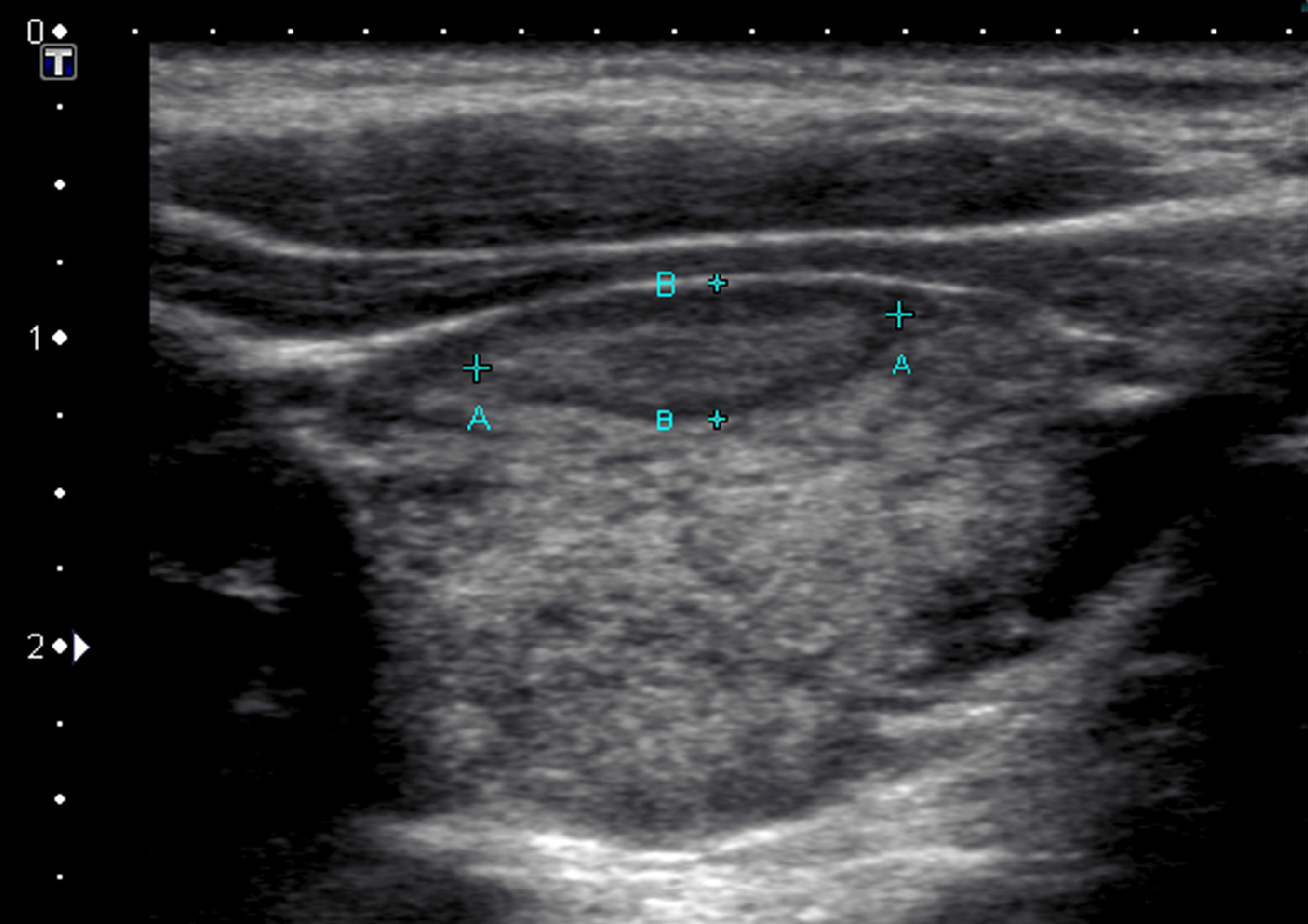
Fig 1. R thyroid reported as nodule
I see many thyroids incorrectly labelled as multi-nodular but at followup the nodules change or disappear as the thyroiditis (almost always Hashimoto’s thyroiditis in this scenario) effects more and more of the gland. This random mixed geography of patchy autoimmune thyroiditis (small hypoechoic “micronodules” mixed with some normal thyroid tissue and some intermediate thyroid) can pop out a simulated nodule. The abnormal colour-flow in this scenario spares the unaffected thyroid.
Use colour doppler routinely and get used to using a standardised setup with a scale of between 5 and 10cm/s. Of course you can vary this but in terms of grading gland vascularity for thyroiditis a standard setup is helpful.

Two years after fig 1 above. Now clearly a patchy thyroiditis. The small hypoechoic zones are NOT nodules.
Micro-calcifications do not occur in echogenic nodules. If you see some get a second real-time opinion. Micro-calcifications can be difficult to differentiate from colloid artifact and very difficult on still images so if the reporting sonologist is nearby ask them to look in real-time. If there a tiny space anterior to the echogenicity it is almost certainly colloid artifact. If there is no obvious colloid in the lesion it is probably micro-calcification.
Cystic spaces and colloid usually indicate a benign lesion (definitely not a 100% rule and unfortunately follicular neoplasms occasionally contradict this rule -but are usually all or mostly solid).
For more information on thyroid nodules.
If you have any tips or questions write to me at info@driainduncan.com.au.