
 Dr Iain Duncan
Dr Iain Duncan
April 2026
2026 has been both interesting and challenging. Something new will be happening at ultrasoundCBR soon, but you will need to wait a little longer. My website is pretty static except for an update on small joint PRP therapy –see here. Our usCBR team continues to work together and we all make each other better. Let us know how we could do better at hello@ultrasoundCBR.com.au.
November 2025
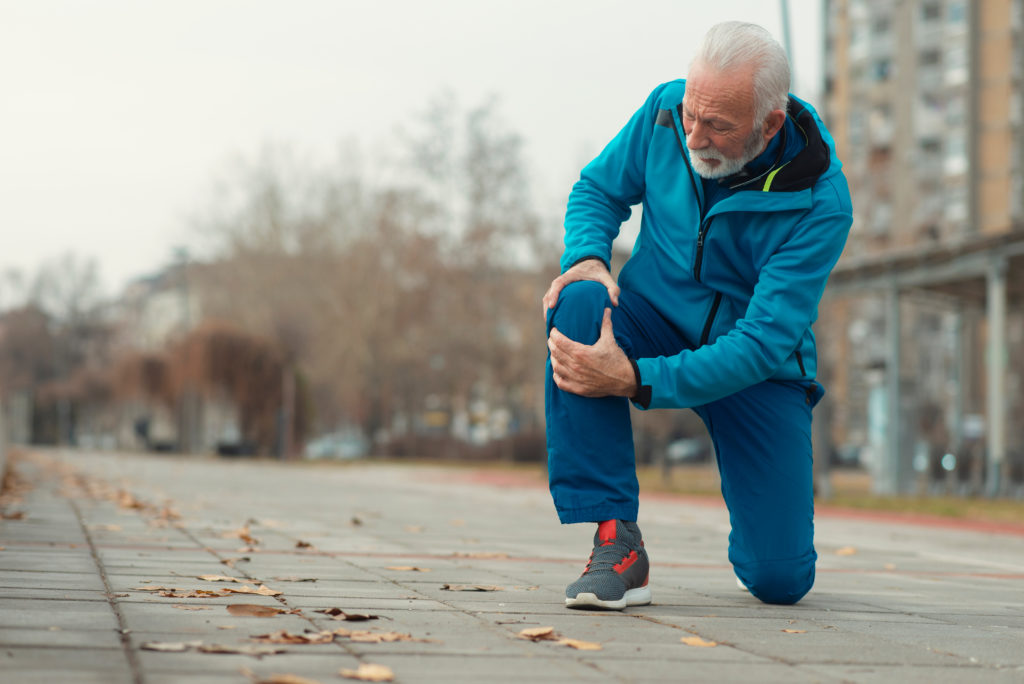
This has been a year of continuous change for me. I have become increasingly involved in clinical assessments and adjusting to a narrower focus: either musculoskeletal assessment (clinical plus ultrasound) or leading an amazing ultrasound team at ultrasoundCBR. I am enjoying every minute. Spending time with an enthusiastic, dedicated, and experienced team has been a joy. The team brings years of experience with a dedication to ongoing improvement and proving the best possible assessment and experience. The office team enables a great patient experience and will do their best to help wherever they can. Also I have enjoyed a new collaboration with Sam at Junee Ultrasound (see photo), which has been both rewarding and fun.
In terms of injection therapy recent evidence suggest Platelet rich plasma is the choice for Carpal Tunnel Syndrome, with 5% dextrose as 2nd preference, and corticosteroid only better than placebo for 3 months (see https://doi.org/10.1371/journal.pone.0303537, https://doi.org/10.1016/j.apmr.2022.11.009, and https://doi.org/10.1002/term.2950)

June 2025
On my departure from GMI I have stepped back from molecular imaging and nuclear medicine to lead the team at ultrasoundCBR and provide this next level ultrasound service. The first six months of ULTRASOUNDCBR have been fulfilling and amazing. The whole team has come together in quite an extraordinary way. There were very few “glitches” and we have pioneered new IT and care delivery systems. Nick Ingold was instrumental in setting up all our systems and employing our amazing staff. He also managed to participate in the “Shitbox rally” to raise funds for the Cancer Council of Australia (see photo), which of course we were delighted to sponsor.
I have now focused fully on delivering the best possible ultrasound service across the whole spectrum of ultrasound scans. In addition the team and I will continue to provide state of the art assessment and interventions for musculoskeletal problems.
I am pleased to see many old friends and patients have found us at Bruce and bring their friendly faces.

December 2024
After a significant break I am starting a new specialised ultrasound and clinical practice in Canberra named ULTRASOUNDCBR which we launched this month. This is an independent practice with specialised skill and experience in ultrasound dedicated to patient centred care. All the sonographers have decades long experience. We have every ultrasound specialty covered. Worth a visit!
June 2024
I am leaving Garran Medical Imaging with some sadness and I apologise to those that may be affected. At this stage I cannot give a date for a return but will post an update when the situation changes.
May 2024
The year marches on. I was pleased to see an article about my work on Tc-PSMA scanning in the North American Publication Medicine Innovates –see here. I attended the ANZSNM conference in Christchurch at the end of April which alerted me to what my colleagues are doing around the country. Nuclear medicine is such a diverse discipline and often we are unaware of progress in areas that we do not directly work. I note there is a massive shortage of nuclear medicine physicians in NZ.
Christchurch city is still full of “voids” post the 2011 earthquake, but gradually new builds are appearing. We also spent time in Lake Wanaka where we were privileged to see the first snow of winter falling (see photo below).
I also welcomed my first grandchild to the world on 19th April. A truly amazing feeling.

March 2024
The Maldives was a great place to spend a week at Christmas, but that was so long ago…
Another year launched and already Summer has nearly finished and the deep delve into fiction and non-medical books is giving way to brushing up on latest findings. Meta-analyses are popular forms of literature review but often lose some of the strengths of the underlying individual studies. By putting multiple studies together we are strengthening the findings about some general interventions, but often looking at the specific differences between studies is as useful as the similarities used to combine data. For example I have added some recent PRP (platelet rich plasma) meta-analyses to the list of PRP references. An interesting note on the meta-analysis of Barman et al was that they chose randomised clinical trials that compared autologous-PRP injections with placebo or another intervention for
persons with shoulder diseases. So any comparator and several shoulder diseases were all considered. Clearly this approach while providing some general information about the utility of PRP, is not the way a clinician would approach a shoulder problem in the real world. The overall effect of PRP therapy was compared to whatever comparator the individual studies used for whatever indication the study included. Of note there were very few placebo studies and in one of the studies which significantly reduced the pool effect of PRP, the comparator was PRP+HA!
As a clinician the details I look for in any given paper are I suspect quite different to a pure researcher. While I respect the importance of academic assessment of published papers, there are many (different) details which as a clinician I look at very closely, so I can understand the differences of approach to my own and therefore sometimes the importance (or not) of the findings. The standardized pain and function measures used in clinical trials are not the same as specific patient reported outcome measures I use as a clinician. Hopefully I will do a full review of our own patient reported outcomes measures (from my PRP patients) later this year.

July 2023
Where to go in 2023? I don’t mean a geographical location but rather a strategic direction. There are so many possibilities for improvement and research in clinical medicine (see some of my recent publications). I collect a lot of data which might not sustain critical academic scrutiny in the conventional clinical trial paradigm as medicine has yet to embrace big data in any meaningful way. I first advocated the value of big data in the very earliest days of office and personal computers (1980’s). I designed a rheumatology database system in DBASE and later Microsoft Access which had detailed diagnostic, treatment, and outcome measures for all my patients. This database profoundly influenced the basis of my early clinical practice (which was paperless before that was a thing). The data I collected allowed me to nuance and develop my treatment of rheumatic disease far more than the published clinical trials. I was sure this would be routine practice across medicine within a decade but here we are 3-4 decades later with still only the beginnings of widespread patient data collection and application. Australia in particular lags behind much of the first world in this respect. Value based healthcare (for more about this visit the Patient Experience Agency) is coming but the sacred cow of Medicare is a block to its implementation in medical practice. Funding remains fixed to episodes of interaction not to provision of (quality) care.
Measuring PROMS and PREMS (patient outcome measures) is easier in rheumatology than Medical Imaging as Diagnostic Imaging (DI) is a single component of multidisciplinary care and shares patient outcome with multiple participants.

Performance in DI is not systematically measured and yet it is a critical part of patient care. Many patients diagnosis and subsequent management are based on DI which has an estimated error rate of at least 5%. Communication between DI specialists and clinicians is often poor and a great deal could be done in this area. We at GMI would love to partner with others to improve this situation but there are so many blocks. Sharing the patient’s clinical data across services would be a start….
April 2023
Returned from another walk in Tasmania, equally as invigorating. Also another episode of Covid (like so many others) despite just having a 5th vaccination. GMI keeps moving relentlessly forward and we try hard to keep at the cutting edge of so many things. Our work on Tc PSMA scans was published this month in The Prostate and I would like to thank all those who have contributed along the way. Well done.

Keep to the path
January 2023
Happy New Year. I have just returned from a wonderful walk in Tasmania. So good that we are already planning our next walk.
Bring on 2023! GMI has a new website and online booking facility for 2023? This should streamline bookings and avoid too much waiting on the phone. Nevertheless we are always happy to talk to you as the more customised we can make your booking the better your experience and outcome. In particular for myself I can provide a consultation service but only if you have a referral for such.
We will be introducing a few new services in 2023 where there is a significant quality gap in the ACT.
October 2022
2022 has been an interesting year at GMI. My co-founder Kevin Osborn has retired and of the original team there are only 4 remaining. We continue to evolve and have recently launched a new website. Our practice is close to functional capacity in the footprint we have at Garran. We have modified several spaces to try and improve both functionality and throughput, without compromising patient care. 2022 looks like the first year where some AI applications are ultrasound ready and I have already had some interesting discussions with developers. We have at this stage decided to go with smart software to improve workflow and efficiency rather than AI applications at this stage, but I suspect that may change in the next few years. Nevertheless at the core of our practice the human element is likely to be enhanced rather than replaced by near-future developments.
The ASUM conference (Australia’s premiere ultrasound conference) in Adelaide in September was a great success and most of our ultrasound team were able to attend. ASUM premiered a new format involving a “deep dive” day which allowed the attendees to spend an entire day on a given topic. In my case I spent time learning a lot more about endometriosis and the team here at GMI have instituted several changes to our protocols to enhance our evaluation and detection of this under-diagnosed condition that affects a up to 10% of women of child bearing age. Endometriosis Australia is a great resource for this condition.
Nick Ingold (GMI practice Manager and nuclear medicine guru)and I also spent time in Vancouver at the The Society of Nuclear Medicine and Molecular Imaging (SNMMI) and briefly in Brisbane doing a theranostics course. The photo below shows it wasn’t all study!
Continuing education never ends! This keeps us on the “edge” here at GMI where we can work together to pass on the latest techniques and understanding to our patients.

July 2022
A recent publication shows an Achilles fat pad steroid injection may help rehabilitation in some patients with mid-Achilles tendinopathy. While the study shows substantial differences between placebo and steroid, many injection candidates were excluded prior to the study which indicates that in the real world this intervention may have quite a restricted practical application.
June 2022
No updates since October so my regular reader will be disappointed. I remain manic at home and work as I really don’t know how to get bored. I’m working on that too. When I’m not actually at GMI I’m working on data (PSMA scans and PRP injection therapy mainly) or reading (medical, fiction, and non-fiction). I do a bit of binge TV watching also (recent binges include anatomy of a scandal, Ozark, and the Lincoln Lawyer). A recent non-fiction that I enjoyed greatly was The Journey of Humanity by Oded Galor which really makes you think about the world differently. Galor looks at human diversity and progress over the entire history of homo sapiens and looks at the “big” influences and determinants of human economic and social development. What he finds is ultimately surprising. It seems that there may be an optimal level of population diversity and that this is linked to migratory distance from Africa. If this tweaks your curiosity I recommend the read.
Our PSMA experience /data up to August 2021 has now be collated and the first paper is in its final stages. Hopefully will be published before year’s end. My PRP injection data is less sophisticated but I may be sharing this with a wider medical audience later this year also. Academic business may be normalizing post covid. Fortunately I suffered only a mild bout of the illness. I’m heading off to the The Society of Nuclear Medicine and Molecular Imaging (SNMMI) conference in Vancouver this month, my first trip post covid. Looking forward to it!
I’m pleased Australia has voted in a new Government, gives us hope for the future. Remember GEM is a universal key (Gratefulness, Empathy, Mindfulness).

October 2021

I have written a new PRP update which highlights the increasing evidence for LP-PRP (leucocyte poor platelet rich plasma) therapy as being the best intra-articular option for knee osteoarthritis in a network meta analysis which compared it with intra-articular hyaluronic acid, leukocyte-rich platelet-rich plasma (LR-PRP), bone marrow mesenchymal stem cells (BM-MSCs), adipose mesenchymal stem cells (AD-MSCs), and saline.
In the world of nuclear medicine and molecular imaging there was an exciting announcement by the Australian Government committing $30million to the design a new world leading manufacturing facility to be built at Lucas Heights in Sydney. This is overdue as the current facilities have been dogged by recurrent failures and breakdowns in recent years, despite the availability of the OPAL state-of-the-art reactor. As stated in the release “[the facility] will save Australian lives, support thousands of jobs and further enhance our sovereign capability in this important area of medicine.”
Radioisotopes save lives
September 2021
There is not a lot to talk about with business restricted to necessities only during our A.C.T. covid lockdown. I added this research to my shoulder list: https://doi.org/10.5414/CP203262 . This supports the use of PRP for shoulder capsulitis or frozen shoulder, and is something I undertook for the first time this month, and only as all other options had failed. This will be a tough clinical test for PRP in a severely frozen shoulder.
I continue to spend many hours every week making sure I am up to date in all of the areas in which I practice. While at times this can be onerous, it is also reaffirming and at times exciting. I discover some gem every few weeks which may improve the way we practice at GMI. Sometimes knowing that we are already ahead of the game is reaffirming but there is no “cruising” in the modern world. Change is a constant. I hope to be the best I can be on the day before I step away from my current role.

June 2021
We are proud to have (again) achieved full diagnostic imaging accreditation at Garran Medical Imaging for a further 4 years. The accreditation process takes a great deal of work and ensures you can expect all our scanning, professional, and diagnostic processes won’t let you down. I have also personally achieved recertification of my Diploma in Diagnostic Ultrasound (DDU) for a further 4 years. While the latter is not a requirement of any regulatory body, it does ensure that I am personally up to date in all the ultrasound field in which I practice.
May 2021
I have been reading the recent reviews and literature on PRP therapy. The Biobridge Foundation has recently published an excellent 180 page summary of 20 years of research (laboratory and clinical) and reviews by leading clinicians in the use of PRP (platelet rich plasma) and HA (hyaluronic acid). This plus other data supports our use of leucocyte poor platelet rich plasma (LP-PRP) as the preferred injection therapy for many of the conditions we treat. I am still trying to finesse the clinical applications of LP-PRP, hyaluronic acid (HA), and combination therapies to try and predict the optimal choice for each patient and clinical problem. While there are a growing number of clinical trials demonstrating their value, the clinical setting for each patient has so many likely important variables, which cannot be adequately studied in clinical trials. Optimizing our protocols and recommendations is in constant evolution which requires ongoing feedback and follow-up. At least in 2021 we can get a lot of follow-up using email and online surveys. Thanks to those who have helped or will help me in this project.
March 2021
 March saw Canberra day, the Balloon Festival, and Enlighten in Canberra. The practice was busy and aside from supply shortages everything is running well. A publication in Arthroscopy showed a better pain response to PRP for partial thickness rotator cuff tears up to 3 months post injection, but no difference at 12 months. Only a single injection of either was used whereas other trials have done more than one injection.
March saw Canberra day, the Balloon Festival, and Enlighten in Canberra. The practice was busy and aside from supply shortages everything is running well. A publication in Arthroscopy showed a better pain response to PRP for partial thickness rotator cuff tears up to 3 months post injection, but no difference at 12 months. Only a single injection of either was used whereas other trials have done more than one injection.
The latest PRP therapy result from Garran Medical Imaging can be found here. I am pleased to say 86% of our patients report a >50% improvement in pain after PRP therapy (for tendon and joint problems), when measured at between 2 and 6 months post therapy.
February 2021
I hope everyone had a “break ” over the holiday season. Mine was belated but restful. I didn’t get to travel being afraid of both rapidly changing Covid-19 restrictions and losing yet another deposit to the inflexible Airbnb. Also we didn’t want to contribute further to the long term housing/rental shortage created fueled by the Airbnb craze.
On the medical front I note a couple of interesting knee osteoarthritis studies. For patients with osteoarthritis of the knee this study suggests a “winner” in the long debated issue of footwear and OA knee. A popular belief among many professionals is that flat flexible shoes improved knee pain but this study found that stable supportive shoes were significantly better, in a head to head comparison with regards to knee pain over a 6 month period. The supportive shoes also showed a trend towards improved function relative to the flat shoes.
Another study looked at comparing a stepped (and online supervised) exercise program with a standard education program. Patients in the stepped program get increased intervention depending on their response to each level of intervention: “The STEP-KOA intervention began with 3 months of an internet-based exercise program (step 1). Participants who did not meet response criteria for improvement in pain and function after step 1 progressed to step 2, which involved 3 months of biweekly physical activity coaching calls. Participants who did not meet response criteria after step 2 went on to in-person physical therapy visits (step 3). The AE group received educational materials via mail every 2 weeks”. Only 35% progressed to step 3. The stepped group had a significantly better WOMAC score (this is a standard overall hip/knee arthritis score) compared with the “control” group.
December 2020
I am now introducing combination PRP injections with hyaluronic acid for osteoarthritis in the knee. This is done using the cellular matrix device, which has only recently become available in Australia. Evidence for this combination comes from these previous studies which showed the superiority of the combination over solo therapy.
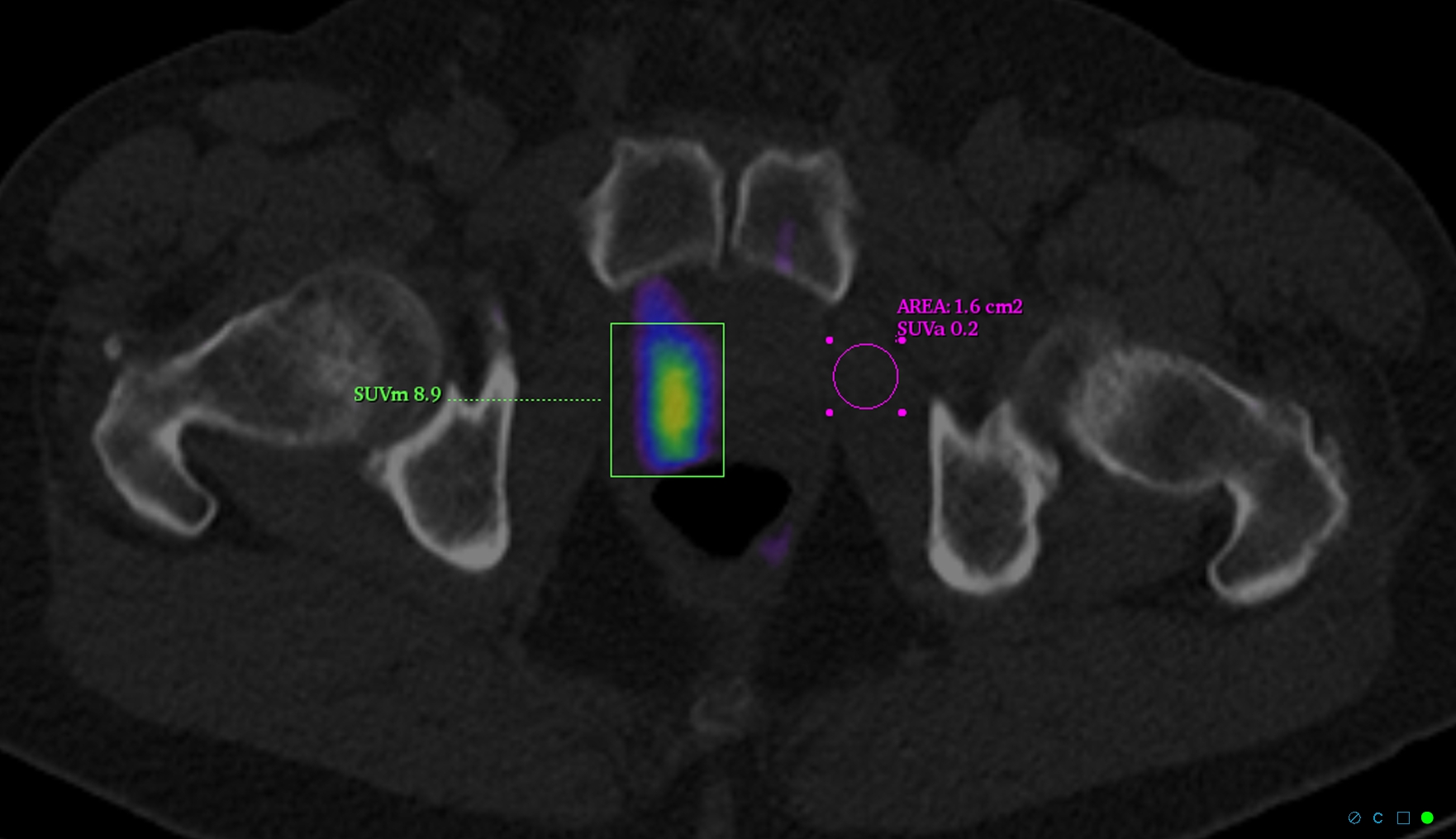
We are doing a lot of PSMA scans this month. For those interested in the underlying evidence, some of the original research is listed here.
November 2020
The holiday season awaits. Are we rushing to get there or hesitantly moving forward? I’m in two minds, having got into a comfortable routine and staying close to home all this year.

This month I was introduced to a new and exciting therapeutic program by Tina McIntosh at Brainchanger.io. This has been a gamechanger for many patients with chronic pain whose pain “systems” have become dysfunctional. It can run parallel with other interventions and utilises modern pain theory to “recalibrate” their pain experience.
I was also able to speak to our local rheumatology group about assessing rheumatoid arthritis with ultrasound and about PRP therapy for knee osteoarthritis.
Both these activities can help raise the bar on effective communication between healthcare professionals. This is as important as the interventions as healthcare can so often be fragmented and difficult for the patient to navigate effectively.
October 2020
Continuing on with the data theme of September (see below), I am overwhelmed by the amount of data that I collect in the course of my work. I have always been a keen data collector designing my first medical database in the 1980s and writing my own practice software for my rheumatology practice in 1990. Over several years I was able to instantly analyze which patients were on which treatments, how they responded, etc. I could view overall response rates and side effect profiles of different therapies across my patient groups. Even today this sort of ongoing analysis is not available in practice software.
I continued with data collection after my move to medical imaging, but while data collection is second nature, getting useful information from the data, clinical follow-up of interventions and scan results is much more difficult. I am currently making a more concerted effort to get better follow-up. So if you get an email, look kindly at it, and thanks in advance for your cooperation.
September 2020
The data space we live in gets larger exponentially every year, and paradoxically data mining becomes more of an art form. We hope that AI will help us make sense of this sea of data. No more is this more evident in Medicine where conventional medical journals are under assault on all fronts. This assault in many ways is both reasonable and predictable, but we need to ensure that the “baby is not thrown out with the bathwater”. It will be interesting to see whether the conventional model and established journal monopolies will make the required adaptations going forward.
For those interested in some staggering Covid 19 data see this article in JAMA.

August 2020
August was our busiest month ever but…

July 2020

Life goes on (despite Covid-19). Fortunately, my work life is little affected, though like many my out-work-life is now quite “confined”, but the upside is I’m saving $ not eating out, and when I do its a (very) special occasion.
PRP therapy continues to generate more and more interest, so I have started a collection of references that have influenced my thinking on the subject, see https://driainduncan.com.au/references-for-prp-therapy/.
There are quite a number of studies that really challenge the accepted dogma that corticosteroid injections are the first choice when conservative management fails. One such from Jane Fitzpatrick and colleagues (an Australian study -see here) showed that patients with chronic gluteal tendinopathy for more than 4 months achieved greater clinical improvement at 12 weeks when treated with a single PRP injection than those treated with a single corticosteroid injection.
I have added new material to the sections Updates on PRP for Osteoarthritis and Updates on PRP for tendinopathies and tendon tears. I note that there is now more evidence supporting a longer-term benefit for PRP with one study [2] showing an average patients’ subjective symptomatic relief of 9 months for HA (viscosupplementation) and 12 months for PRP (platelet-rich plasma).
June 2020
I was supposed to be delivering a lecture this month on Quantitative SPECT: From Theory into Practice at the (North American) Society of Nuclear Medicine and Molecular Imaging in New Orleans, but unsurprisingly I am not. Instead, I am spending my time bike riding and walking the streets of Canberra and the tracks around Lake Burley-Griffin. There is still plenty of building activity in Canberra which has not been affected by Covid-19. Constitution Place (right) is starting to look spectacular.
May 2020
Work rebounded in May with plenty to do at GMI but the ANU and its Medical school remain closed. (Alas) I did not get to present my 3 abstracts on Tc-PSMA in prostate cancer at the ANZSNM conference in Sydney, but no doubt I can present the data at another forum or even publish it (time willing).

April 2020

It was pretty quiet at work as a result of the Covid-19 lockdown. Still a chance to focus on what matters most.
New to the site are some of the American Academy of Orthopaedic Surgeons’ recommendations for the management of rotator cuff tears.
Meanwhile, in Canberra, I caught up with John Curtin and Ben Chifley who like many older statesmen were exempt from the social distancing rules.
March 2020

I have recently perused the 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee published in Arthritis and Rheumatology in January. While I agree with more than 90% of the recommendations there are a few I believe are conservative and ignore some pretty good evidence in favor of the status quo -most particularly those regarding intra-articular hyaluronic acid (HA) and Platelet-rich plasma (PRP) injections. The recommendations are based on a consensus from experts within the American College of Rheumatology and Arthritis Foundation after a review of the literature. In regard to specific recommendations, they do not provide a formal analysis or rarely list the pivotal literature. Though generally recommending against HA the guidelines state: “In clinical practice, the choice to use hyaluronic acid injections in the knee OA patient who has had an inadequate response to nonpharmacologic therapies, topical and oral NSAIDs, and intraarticular steroids may be viewed more favorably than offering no intervention, particularly given the impact of the contextual effects of intraarticular hyaluronic acid injections (38).” The guidelines also capitulate with the longstanding belief that IA steroid injections have a better evidence track record: “In OA generally, intraarticular glucocorticoid injection is conditionally recommended over other forms of intraarticular injection, including hyaluronic acid preparations. Head-to-head comparisons are few, but the evidence for the efficacy of glucocorticoid injections is of considerably higher quality than that for other agents.” I believe this statement is incorrect and that evidence standards were simply lower 30-40 years ago, when the steroid lore was established. When you go back and carefully scrutinise the evidence, the study designs are no better than recent studies of HA and PRP. Indeed this study from Gormeli et al (2017) of HA and PRP into knees is as good as it gets (randomised, double blinded, and placebo controlled) -see my brief analysis here. Furthermore, this meta-analysis provides further evidence of the benefit of PRP and HA in osteoarthritis. The guidelines make no comment as to how they come to their recommendation regarding PRP, which I suspect remains in the too difficult category for analysis.
Most of the patients referred to me with osteoarthritis for intra-articular injection have failed almost all the standard recommended therapies and are either too old or too young for joint replacements. It would be hard to refuse therapies to these patients with significant pain and dysfunction on the basis of ACR guidelines, particularly where the risks are lower than with corticosteroid and the potential benefit probably higher.
January & February 2020
Summer has been a troubling time this year with ongoing bushfires, perpetual smokey haze, extraordinary temperatures, and later the spectre of a novel coronavirus. In some way, these have affected us all and make it hard to adopt the “business as usual” attitude. Even when I “escaped” to the south island of New Zealand (for a family wedding) the smoke from Australia was evident on several days. Still, the pack rafting was both hard work (carrying the raft upstream) and exhilarating (paddling it down again).

Like many, I have been filled with some existential angst about wanting to take some action to reduce mankind’s impact on the planet but believing I can make little difference. I also tell myself that I can work best where my skills lie, by helping those patients who come through our practice. There is much to be done in achieving better health outcomes in a caring and sensitive way. I usually focus on the technical and clinical aspects of my practice, but I am aware of how much more (holistically) is needed to provide better care. For those who really want to learn more about patient-centered care I recommend reading Patients For Life by Shelley Thomson.
So every year there are new challenges, some expected and some not. I will endeavor to take most of them on (or ask others to help), which is a recipe for being busy, but will it be productive? Some of what we do at GMI is generally not available in many parts of the world or even Australia. I believe I should spread our experience and (perhaps) wisdom, but in practice, it is hard to do from a small, busy, single practice. This year I have submitted 3 abstracts on Tc-PSMA in prostate cancer to the ANZSNM conference in April and have agreed to give a lecture on Quantitative SPECT: From Theory into Practice at the Society of Nuclear Medicine and Molecular Imaging in New Orleans in June (SNNMI 2020). Hopefully, like my trek in NZ, if I cover the hard yards upstream then these activities will have a significant “downstream” effect, even if not for a few years.
December 2019
The holiday season is upon us again, but December often turns out to be frantic before Xmas. I recently spoke at an education evening about Tc-PSMA in prostate cancer, and I include a window into our experience here. I am hopeful that I will cobble at least some of the data together for either a publication or at least an abstract at the 2020 ANZSNM meeting in Sydney. However, it is likely this project will be competing with others for attention in the 2020 year. As the popular Mark Manson (Everything is F*cked) said (and I may be paraphrasing) “freedom is the ability to choose your pain.”
November 2019
An update on liver elastography.
A publication in Radiology Online cautions us about significant complications following intraarticular corticosteroid injections for osteoarthritis, though the authors do concede these case studies do not necessarily imply causation. The phenomena of accelerated OA progression, subchondral insufficiency fracture, osteonecrosis, and rapid joint destruction can all be seen in patients with OA who have not had injections. Sometimes they are misdiagnosed as OA and have an injection before the recognition of the diagnosis.
October 2019

I am saddened that due to circumstances beyond my control I will no longer be traveling to Bega and the South Coast. This ends a long relationship with many people, staff, and doctors on the far South Coast. Recently South East Radiology was purchased by the Qscan group and new management has elected not to continue with the existing service arrangements with GMI (Garran Medical Imaging).
A big thanks go to all those who worked with me at Bega over the last decade -your support and kindness were greatly appreciated. I hope to keep in touch with many of you. Of course, any patients who would like to journey “up the hill” to Garran Medical Imaging are most welcome.
On another note, a recent meta-analysis shows there are only 4 factors that have been found to predict the progression of hip joint osteoarthritis. To some extent, these are not surprising and 3 of them correspond to the x-ray appearance of the hip (an x-ray is still a valuable tool). The fourth factor relates to co-morbidity, ie general health of the individual.
I will be talking at both the ANZSNM Capital Region Forum and the ASA SIG meetings this month. The former will be a lecture on xSPECT/CT bone and the latter on rheumatology ultrasound, both subjects I can get a little passionate about…
September 2019

Winter has been invigorating here in Canberra and it is always with some trepidation that I anticipate the Spring Allergy season.
For those interested in xSPECT/CT bone imaging my lecture at the World Molecular Imaging Summit is now online here.
For those with chronic pain, there is a great new system and management resource at Brain Changer.
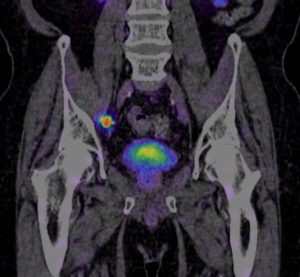
We are now importing our Tc-PSMA from Hungary and have noticed a significant improvement in image clarity. It is very clear that these scans are having a significant impact on therapy for prostate cancer.
I was impressed by a recent paper on PRP and viscosupplementation injections for rotator cuff tears –see my comments here. I believe there is sufficient evidence to offer these injection options with some confidence about improving outcomes for patients with these smaller cuff tears, which (untreated) often progress over time. Check out the evidence for yourself here.
June 2019

I hope 2019 is going well for you all. As you can see from the lack of updates it has been pretty busy for me. Professionally my life is “full” and my personal life is fulfilling but mostly supports my busy professional life. Can’t always separate the two -sometimes that’s good and sometimes not. For those who are interested in mental health, anxiety, and the dysfunction spreading through western liberal democracies I suggest the following are excellent reading: Lost Connections by Johann Hari, and Australia Reimagined by Hugh Mackay. Though these are two very different books the reader will immediately see a common underlying thread in terms of the epidemic of anxiety/depression within our (lack of) communities.

I have been able to make time to attend the ANZSNM annual conference in Adelaide and travel to speak at The World Molecular Imaging Summit hosted by Siemens in Lausanne, Switzerland. The latter provided a great excuse for a (well deserved?) break in Northern Europe (Switzerland, Germany, Czech Republic, and Norway). The Norwegians do interesting modern apartments (see photo) and have lots of electric cars.
My talk on xSPECT/CT bone in Lausanne was very well received and reinforced to me that what we do at Garran Medical Imaging is really the cutting edge in bone scan technique. I will share the link to my talk if and when it is available online. While the science is complex and obscure for most (both patients and doctors) I have seen how it is really making a difference at the clinical level. It was a great pleasure to present the GMI experience (in Switzerland) to an appreciative audience.
I am hoping to spend some time in the latter part of 2019 reviewing our extensive data that we are continuing to accumulate in various research projects, but I’m not so good at looking through the data as accumulating it! I need some help there.
December 2018
I have been invited to participate in Siemens World Molecular Imaging Summit in Switzerland next year, a great honor for me and an accolade for the high-quality work we are doing at Garran Medical Imaging. I will be sharing my experience with xSPECT/CT bone scans in the arena of musculoskeletal medicine with our molecular imaging leaders from around the world.

2018 has been another in which I hope we have continued to serve our patients and referrers with world-class service and medical imaging. Particular medical communities we have made special efforts for in 2018 include long-term renal patients (dialysis patients and those on the transplant list), rheumatology patients, those suffering from prostate cancer, and those with chronic musculoskeletal disorders. If you think we can help, please email us at admin@garranmedicalimaging.com.au.
I have and will continue to travel to Bega to provide cardiac testing and medical imaging support to the region. I was delighted to talk and catch-up with many local practitioners about my experience in Prostate Cancer Imaging and Diagnosis. This took place in colourful Merimbula, in October this year. I hope it was a helpful update in a rapidly changing field.
November 2018
I can’t believe Christmas is nearly here. The last few months have been busy enough to prevent me from doing any updates! Garran Medical Imaging and our work with xSPECT/CT bone has been noted at several “locations” around the globe, such as in Medical Imaging Life -see the online article here. Mostly the latter part of this year has been about consolidation and improvement rather than the new stuff. Collecting data and refining our systems so that we can be sure we are delivering the world’s best care.
I have noted increasing referral for articular therapies for Osteoarthritis -mostly for PRP and viscosupplementation (eg. duralane, synvisc and monovisc). These therapies provide additional options for those suffering from significant pain related to their osteoarthritis. All of the options are safe but involve some cost to the patient with limited and variable health fund reimbursement. The clinical response are very mixed, but for some the result is quite amazing, with surprising improvement seen on scans in parallel with clinical changes.
Our Tc-PSMA scan data is also accumulating and some initial data is being looked at by the urology registrars at The Canberra Hospital. We have improved our scan parameters substantially over the last two years and I am proud of the technical results. I am sure local analysis of the clinical data will go a long way to improving the management of prostate cancer, and ultimately outcome for patients both locally and elsewhere. Hopefully some publications may result in 2019.
July 2018
New to the site: Osteoporosis screening tools and links to recent recommendations.
June 2018
June has been filled with chores and commitments and challenges that I’d rather not deal with, but alas are part of life’s administrative burden. The winter in Canberra has made Cairns feel so long ago. I have been able to maintain great fitness with my HIIT (High intensity interval training) and hopefully this might delay my inevitable ageing according to a recent article in The Guardian.
On the professional front I’m seeing some commentaries spring up about xSPECT bone imaging which I hope means it will be more widely adopted around the globe. It is gratifying to see our research reaching afar. More about xSPECT bone can be found on Siemens website here. When combined with xSPECT quant this provides and much more reliable and detailed imaging landscape to assess our patients and referrers diagnostic and management problems. We continue to have great success solving cases which have proven elusive using more conventional nuclear medicine techniques (both for bone and parathyroid imaging). I am hopeful that as more and more medical imaging practices use the technology the data generated will bring new insights and clinical understanding.
May 2018

I have spent some time in Adelaide, Melbourne, and Cairns during April. A mixture of business and vacation. It has been refreshing and educational. Our poster from the WFNMB Melbourne conference was on quantitative bone imaging and how it can improve and standardise the quality of reporting in nuclear medicine. The poster can be viewed here.
The symposium in Cairns was on imaging and therapy for prostate carcinoma. This had some of the foremost experts in the World and I learnt a great deal, which I can put into practice immediately. Managed to fly over the reef in a small helicopter (see my photo right) which was one of the highlights.
My time in Adelaide was a nostalgia trip visiting some old haunts including Goolwa Beach (see photo) and McLaren Vale. Drove past The Queen Elizabeth Hospital where I did my rheumatology training so many years ago….

April 2018
The 12th World Congress of the Federation of Nuclear Medicine and Biology is taking place in Melbourne later this month and I am looking forward to it. I will have a Poster on xSPECT Quant (Siemens Healthineers) which will hopefully generate some interest. This technology is reshaping the way we do our scans and together with xSPECT makes nuclear medicine in general and bone scans specifically much more precise. Though this technology is not widely available I am hoping our experience will convince others of its substantial clinical benefits.
March 2018
Nicholas ingold and I celebrated publication of our study “The clinical value of xSPECT/CT Bone versus SPECT/CT. A prospective comparison of 200 scans” in the European Journal of Hybrid Imaging. This was the culmination of a lot of hard work and data collection and demonstrates how it is possible to undertake quality research in a private practice setting. It is been important for us to contribute in as many ways as we can to improving medical care. In addition it helps us confirm the validity of our practices. When we adopt new techniques we to look carefully at existing research and where it is not sufficient, we try and collect our own data, or undertake our own research, to support (or refute) our current practice. We have fun too.
February 2018

January was quiet in Canberra (as usual) which is a great way to start the year and collect your thoughts. I have used the available time to collect our research data, to analyse some interesting cases, and to add to this website an update on PRP therapy for osteoarthritis of the knee. For those with osteoarthritis there is also recent evidence that topical non-steroidal anti-inflammatory drugs (NSAIDS) can be effective for some, and are safer than oral equivalents.
The update shows convincing evidence of its benefit. I also read the The Checklist Manifesto: How to Get Things Right, by Atul Gawande. This is definitely recommended reading for health professionals and shows how far we have to go in placing the patient at the centre of healthcare.
December 2017
The end of another year. Some landmarks for myself and Garran Medical Imaging in 2017:
A 97% satisfaction rate from our patient feedback.
80% of patients benefitted from their tendon or joint PRP therapy.
Introduced routine quantification in nuclear medicine studies -presentation about this coming at the 12th World Congress of the World Federation of Nuclear Medicine and Biology in 2018.
Passed 1000 liver elastography assessments (and did not charge a separate fee for this service).
Presented our xSPECT/CT Bone data at the ANZSNM meeting in Hobart in April.

And some firsts…
The first 40 Technetium PSMA scans in Australia
The first full study on xSPECT/CT bone in the world (in press for publication early 2018)
The first Australian practice to be featured on the European Society of Hybrid Imaging Website
I am proud to be part of an amazing innovative and committed team who provide service to the best of their ability. Their dedication to ongoing learning, patient service, and helping me with anything I throw at the them inspires me. Our shared priorities at Garran Medical Imaging go something like this:
Our priorities are friendship, adding value to people’s lives, having fun, solving problems, self-improvement, and only then making money.
We had a great year and we plan to do more of the same next year. I hope everyone has a great 2018. Seasons greetings.
November 2017

Our (myself and Nick Ingold, Garran Medical Imaging) research paper on xSPECT/CT bone scans has been accepted by the European Journal of Hybrid Imaging and hopefully will be in press soon. We have also submitted an abstract on Quantitative nuclear medicine for the 12th World Congress of the World Federation of Nuclear Medicine and Biology in 2018. I am proud that we can undertake research, try new techniques, and provide a great clinical services in a small private practice. This helps us stay at the cutting edge and provide the best possible care for those that chose to use our services. We will look after you!
On the website I have posted an abstract re corticosteroid injections for osteoarthritis of the knee. The study findings more or less mirrors my years of clinical experience with this intervention -the benefits are short term and generally more effective for milder degrees of OA. No one has yet directly compared corticosteroid, viscosupplementation, and platelet rich plasma injections all of which are used in similar clinical settings. Generally a pragmatic approach is taken for treating OA knee which includes mostly “try and see” for each of the available injection options, as well as other symptomatic options (analgesia, NSAIDs, acupuncture). Everyone should be encouraged to do regular quadriceps exercises.
October 2017
The last two months have been busy. Mostly finishing and upgrading our study on xSPECT bone -making it (we hope) of sufficient standard for publication. Also on PRP therapy (both undertaking injections and reviewing the literature). An update on therapy for lateral epicondylitis has been added to the website.

The latter shows that if any therapy is required for lateral epicondylitis (common extensor tendinopathy and tears) then PRP injections is the preferred option.
We also has some visitors from “over the ditch” (New Zealand) who came to learn about PSMA SPECT/CT which is an attractive option in NZ where PET scans are expensive and generally not covered by the healthcare system. We have now done about 50 scans and they are living up to our performance expectations.
August 2017
I was delighted to see that the first publication from the Australasian Radiopharmaceutical Trials Network has arrived and can be found online here. ARTnet supports multi-centre research in Australian Nuclear Medicine and is a joint initiative of two organisations that I am a (proud) member of, the Australasian Association of Nuclear Medicine Specialists and the Australian and New Zealand Society of Nuclear Medicine Ltd . It was established several years ago to address the need for a formal research network in Australia for a collaborative, multicentre clinical trials utilising radiopharmaceuticals for imaging or therapy.
The trial shows the clinical value of PSMA PET scanning in the management of prostate cancer. While PET PSMA remains difficult to access for many I am confident that our recently introduced xSPECT/CT PSMA scans at GMI can prove equally useful.
We have been working hard on these since we started earlier this year (see March 2017 below), and can now produce outstanding quality images. Based on experience in Germany and several early publication (eg from New York Presbyterian ) the Tc-PSMA is providing equivalent results with a very high sensitivity and specificity for prostate cancer. For those of you who wish to know more about PSMA I will, eventually, write some more about it from a patient’s perspective. There is a brief introduction at Garran Medical Imaging.
I have also updated my post about PRP therapy for osteoarthritis after 2 years more of experience and journal monitoring.
July 2017

I didn’t spend much time on nuclear medicine in July as I was best man at my brother’s wedding in Scotland. It was an awesome, auspicious, and joyful event that I thoroughly enjoyed. The summer weather wasn’t kind but the scenery spectacular.
June 2017
I have updated my article on back pain and bone scans following belatedly following the publication of an article showing the utility of SPECT/CT bone scans in the clinical workup for patient with lower back pain. The practice at Garran keeps me challenged but I am off to Europe for three weeks!
May 2017
A recent publication in Clinical Nuclear Medicine demonstrated that 99mTc-MIBI SPECT/CT enhanced the performance of conventional imaging for renal tumours, improving the characterisation of benign v malignant lesions and lowering the possibility of misclassification. They demonstrated that sestamibi (a tracer usually used for myocardial and parathyroid scans) has an avidity for oncoytomas but not renal cell carcinomas and this correctly predicted benign lesions pre surgery. For more information see the original article here and they Auntminnie article here.
Also from Auntminnie this month a brief comment regarding an industry-supported study of more than 600 adults with knee osteoarthritis in five countries showed that compared with placebo with a daily dose of pharmaceutical-grade chondroitin. The latter improved pain and function as much as the anti-inflammatory celecoxib. At the 1-month mark, celecoxib improved symptoms the most, but by 6 months both were similarly effective. Chondroitin is widely available and is becoming a useful adjunct in the management of knee osteoarthritis. The mainstay of early to moderate OA (more about the stages of OA knee here) of the knee remains quadriceps tone/strengthening, simple analgesia, and sometimes viscosupplemenation or PRP -more information for patients here.
April 2017
I draw your attention to two recent publications that concern osteoarthritis of the knee. Published in the Journal of the American Medical Association the first study shows that frequent intra-articular steroid injections do accelerate cartilage deterioration. The second in Radiology confirms that those “who lost weight over 48 months showed significantly lower cartilage degeneration, as assessed with MR imaging; rates of progression were lower with greater weight loss.”
I presented my data on the first 200 cases of xSPECT bone at the Australian and New Zealand Society of Nuclear Medicine meeting in Hobart this month (abstract O60). A summary this research can be found here.
March 2017
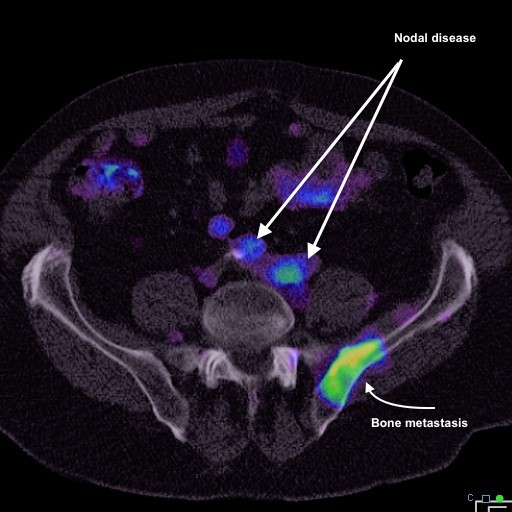
Diagnostic Imaging in Canberra took a leap this month when Garran Medical Imaging undertook Australia’s first Tc-PSMA scan. This will be an invaluable adjunct to assessing and managing prostate cancer. Currently it is available only under the patient special access scheme but we can aim to get approval and import the tracer within 1-2 weeks following a request. We are able to use our direct quantification to assess lesions both for diagnosis and for response to therapy.
I read an amazing book PEAK –Secrets from the new science of expertise, by Anders Ericsson and Robert Pool. I don’t generally recommend books to a wide audience but this is something everyone should read. It turns so many accepted dogmas on their heads and does it using years of research and some very careful observations. I wish I had read it when I was young, but of course it wasn’t written then! Certainly teachers and anyone trying to push themselves should read this. It is quite uplifting and empowering.
February 2017

The year has moved into full-swing this month. Managed to get the years travel planning and data collection in order. I have found the memento database a great tool for data collection and/or creating reference databases. This allows you to create a database entry “app” on you android phone which you can synchronise with others and with google sheets. The latter allows you to collect data for later analysis and to update entries on a recurrent basis (for me that means subsequent treatments, visits, or scans).
February was also full of hot days and spectacular sunsets.
As a small operator in a field where large corporates and giant businesses are the norm I take some solace from the following equation (where did I read this?):
LONGEVITY + DOMINANCE = INNOVATION x GOVERNANCE

The dedicated small team at Garran use the excellent advantage we have on the right side of the above equation to compete effectively in a relatively crowded marketplace. We have clear advantages in innovation and customer/patient services and are still able to offer a better price than our larger competitors. On the innovation side we have several specific projects in 2017:
- Use of PRP therapy for unhealed split tendon tears and osteoarthritis
- xSPECT bone in musculoskeletal imaging
- Intrinsic elastography in the evaluation of tendon pain
- Shearwave elastography for liver disease
- Assessing response to denosumab (Antiresorptive) therapy in metastatic bone disease using quantitative bone imaging
- Evaluating Tc-PSMA in staging prostate carcinoma
January 2017
I really enjoyed a low key Christmas and New Year. I had a chance to reflect on the highs (and lows) of 2016. I think most of us take time out during the holiday season and as I write this I am feeling that gnawing feeling that I need to start doing 2017 things. My whiteboard has been cleaned and the multiple tracks I intend to follow for 2017 are in place. So now I need to start. That means designing a lot of new tools for data collection, considering what abstracts to write and what meetings to attend, and planning any overseas trips. Our modern professional lives are information rich and time poor. Over commitment is easy and though there are useful suggestions to follow we inevitably underestimate the time commitment each project or activity requires. Annie Gibbins has some useful tips but I’m still left with the problem that I enjoy and find rewarding a long list of activities.


Reflecting on 2016 I acknowledge that the amazing xSPECT bone technology I use remains in the “wings” and that its clear superiority over conventional SPECT remains underappreciated by the professionals and patients who might most benefit. Most medical breakthroughs and new technologies have slow uptake and of note my life partner Shelley is no stranger to my “impatience”, particularly in traffic. The benefits are self evident -see images comparing SPECT and xSPECT of the same slice in a C2 vertebra. The pathology is clear in the xSPECT image and remains undetectable in the SPECT image. I have submitted an abstract on xSPECT bone scanning for the ANZSNM scientific meeting in April, which may keep the professional interest growing.