
Bone scans of the spine have become a clinically useful part of the evaluation of back pain. Uptake seen on a SPECT-CT correlates with metabolic activity in bone and the increased resolution and specificity of SPECT-CT has allowed a greater number and variety of clinically relevant findings. Most patients with back pain will have an abnormality on high resolution xSPECT-CT bone scan. Many of these will be clinically relevant and like all bone scans it is sometimes the negative scan that is most helpful.

Intevo xSPECT bone scanner at Garran Medical Imaging
A recent randomized double blind study by Jain et al1 showed that a bone scan with SPECT-CT improved the clinical workup of patients with low back pain by improving the accuracy of identifying the pain source in a group of 80 patients. The outcome from pain blocks was improved and in a small number of patients it enabled critical diagnoses that changed management entirely.
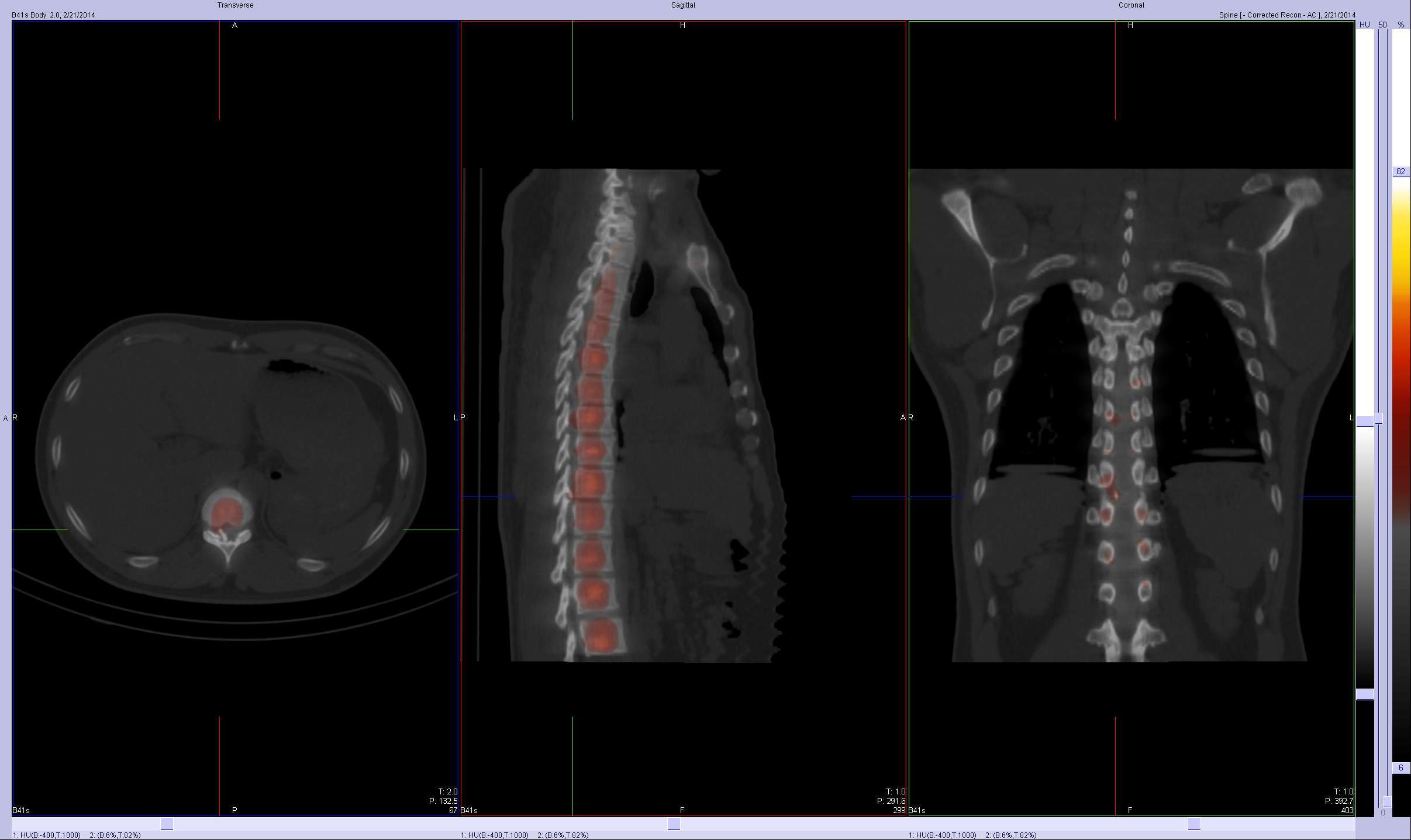
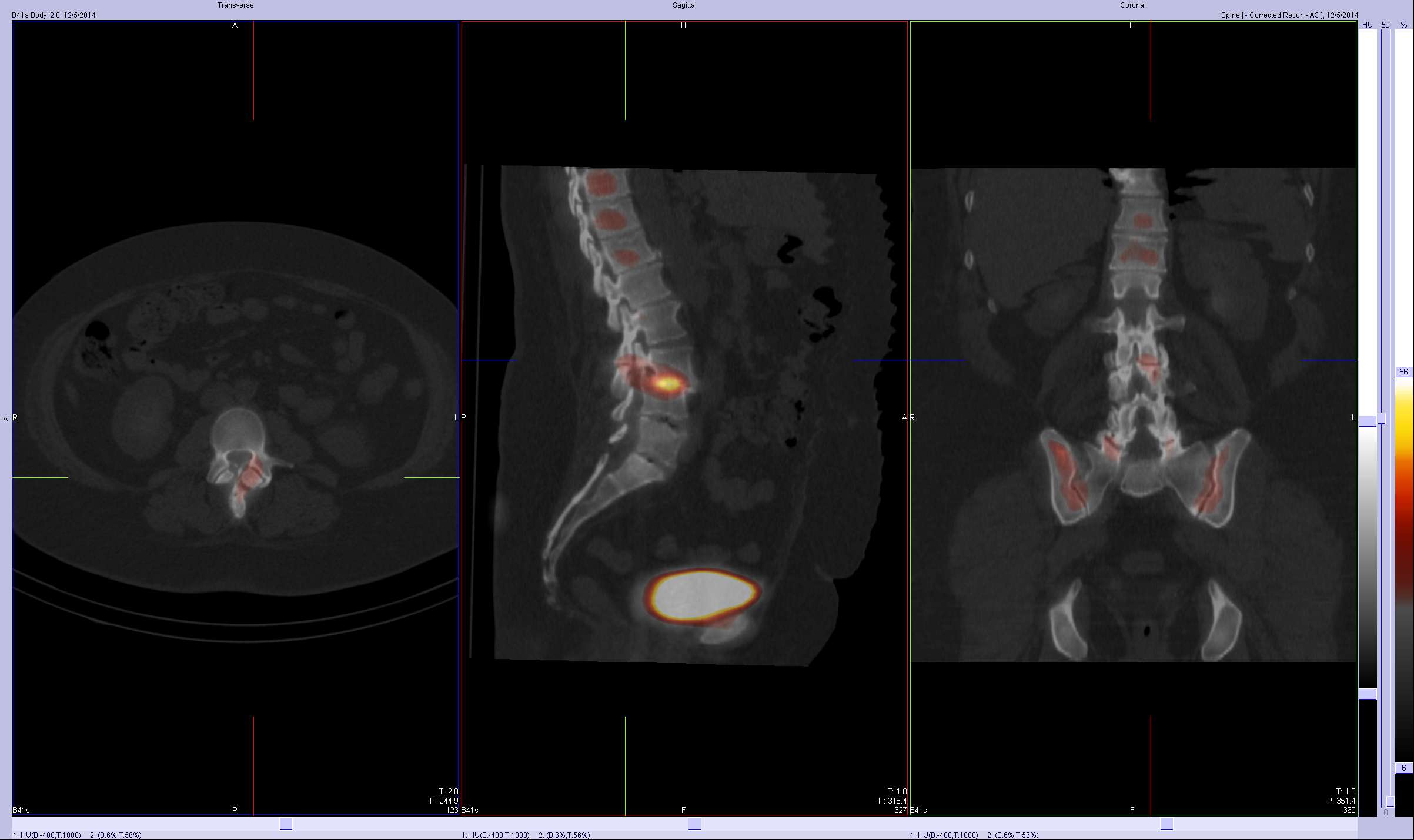
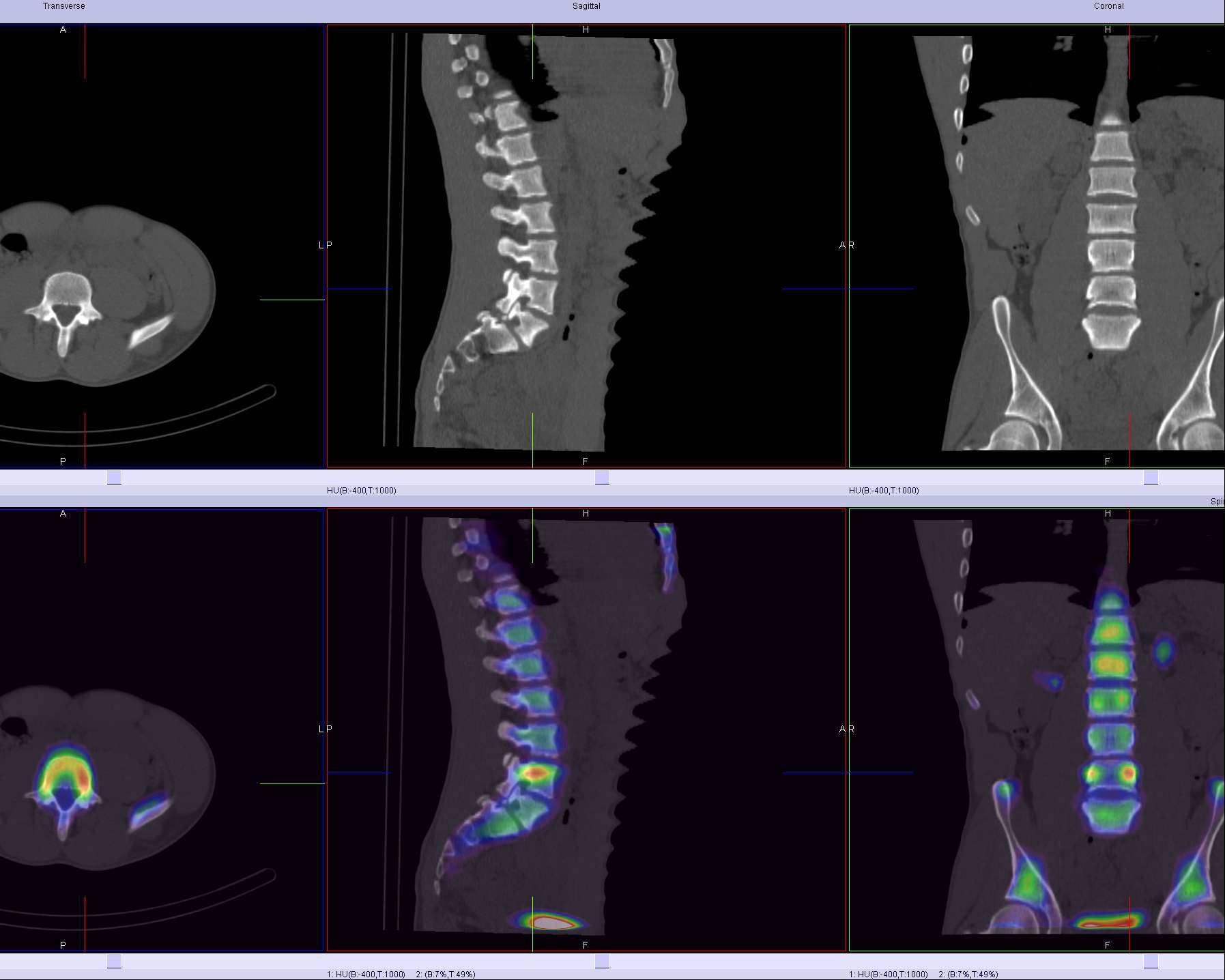
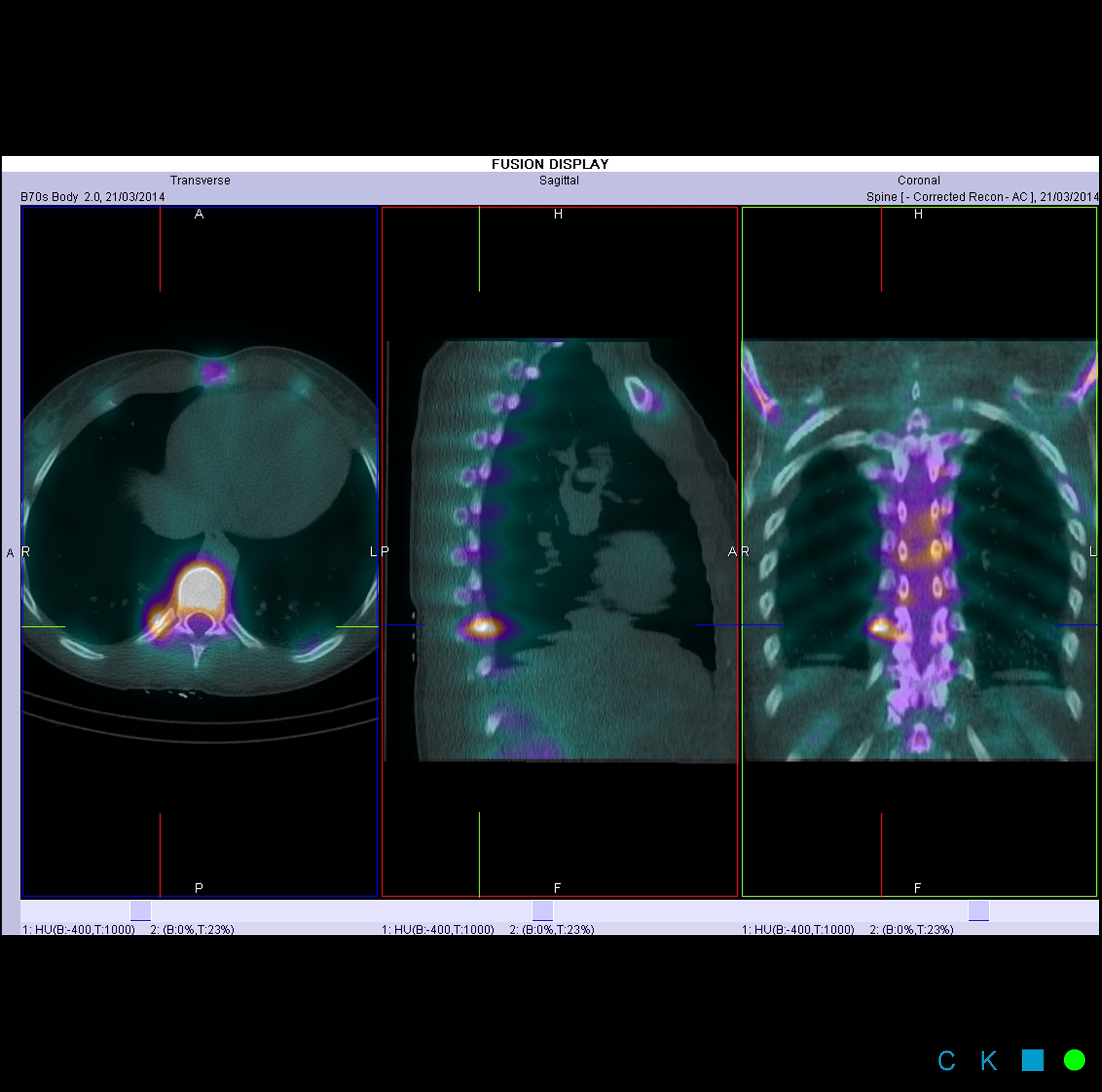
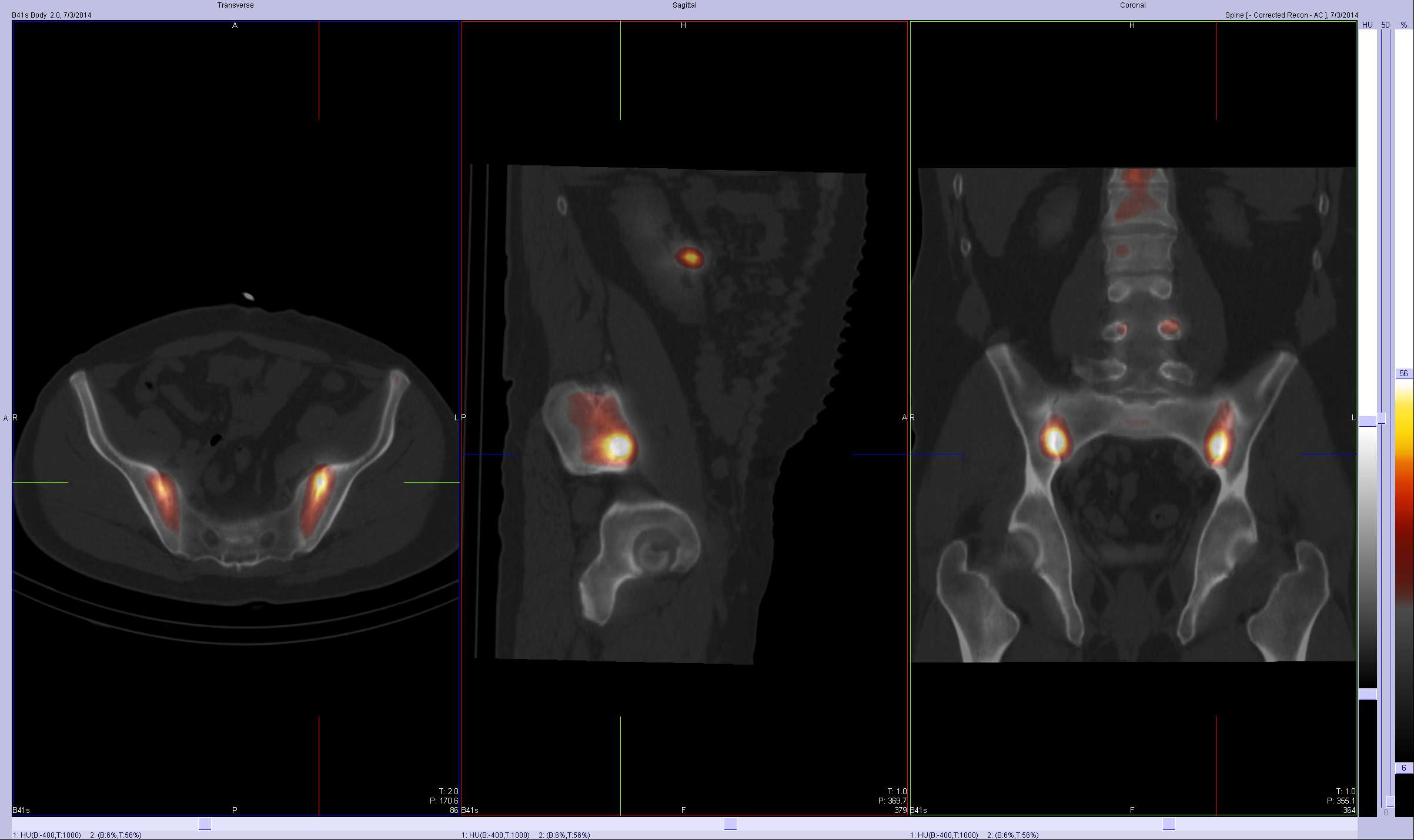
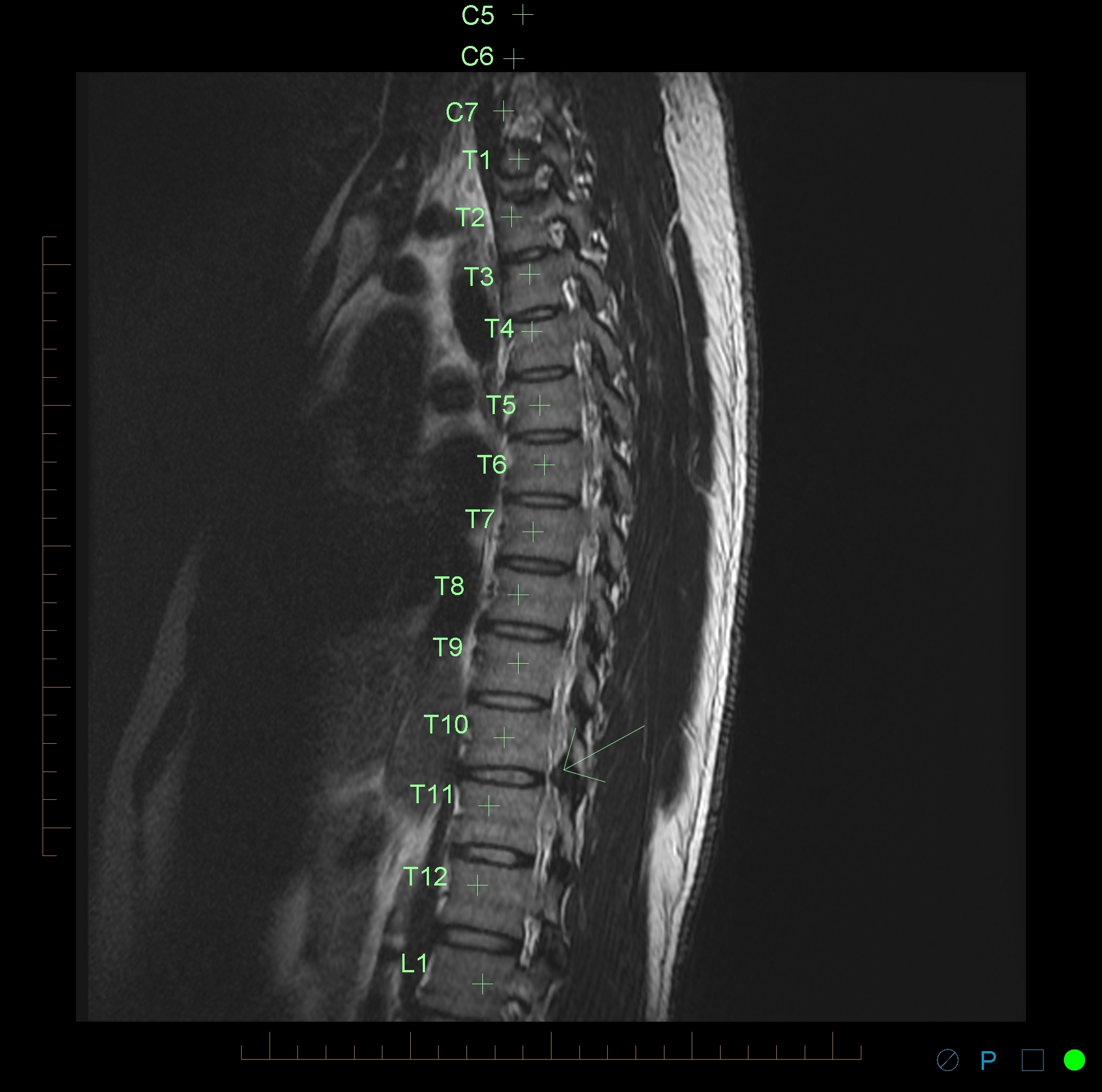
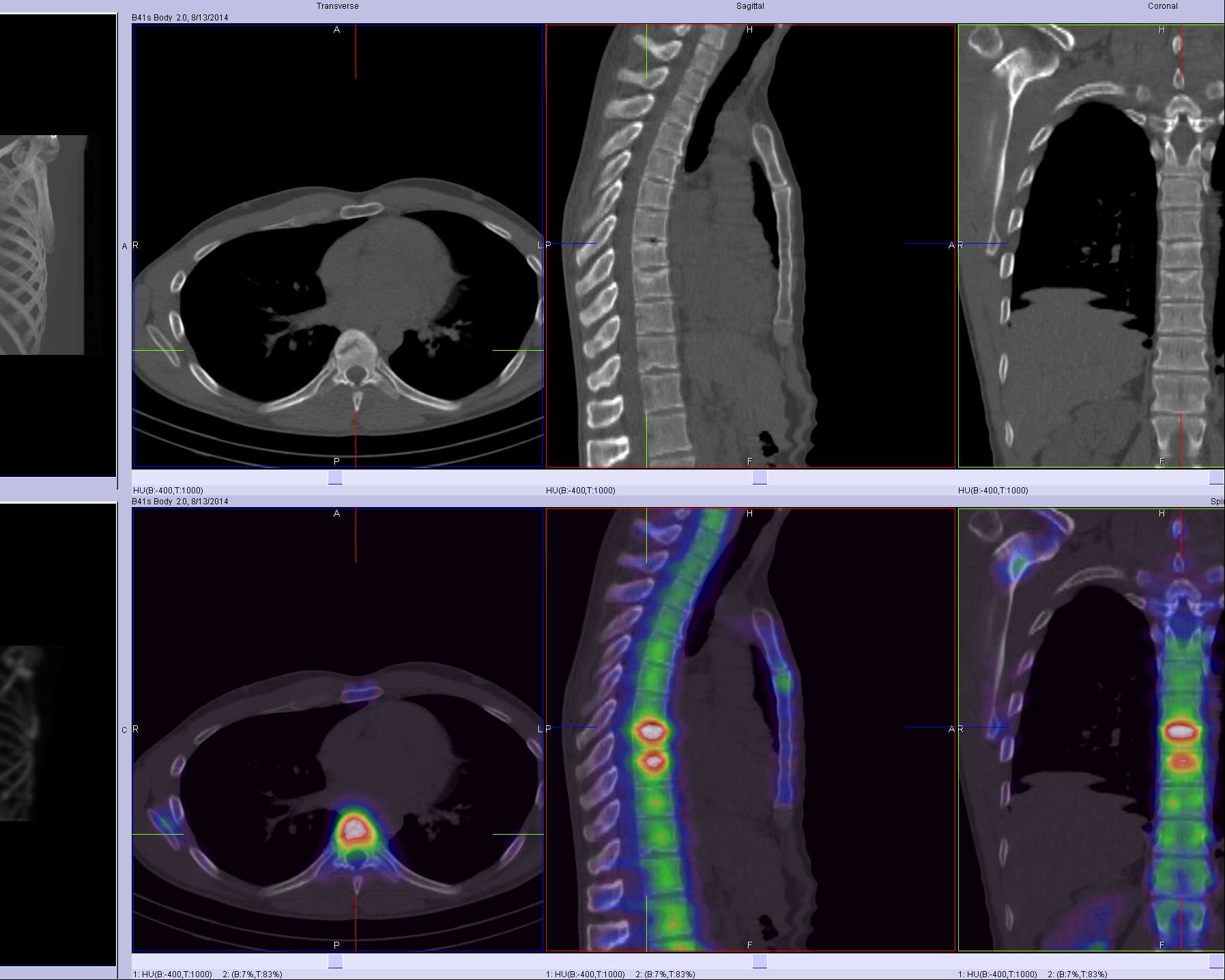
My experience with xSPECT-CT shows that it improves the diagnostic accuracy even further, particularly in relation to thoracic and sacroiliac pain. The image below shows the detail available with xSPECT-CT in the thoracic spine.

Costotransverse and opposite thoracic facet joint arthrosis
The following diagnoses are best made or excluded using a bone scan:
- Active facet joint arthropathy (as opposed to inactive disease which CT and to a lesser extent MRI show anatomic rather than functional changes)
- Significant pars interarticularis fractures (MRI false negative 10%) in young patients
- Fractures
- Bridging osteophytes
- Stress fractures
- Vertebral fatigue fractures
- Boney metastasis (though early lytic disease and lesions less than 5mm are often only seen on xSPECT-CT rather than SPECT-CT)
- In prostate carcinoma suggest bone scan if PSA>10, symptoms, Gleason score >7
- In breast carcinoma suggest bone scan in recurrent breast cancer or stage III,IV disease
- Post surgical fusion complications (>12months post surgery)
- Fusion failure -cold on scans done early post surgery (<8 months) and hot (>18months post surgery)
- pseudarthrosis
- adjacent segment disease
- screw impingement
- Transitional vertebra with partial incorporation stress injuries (not seen generally on MRI)
- Sacroliliitis
- Sacral, coccygeal and pelvic fractures
- Enthesitis at the adductor attachments, greater trochanters,
- Pseudarthrosis between joint variants (partially incorporated vertebra) or between posterior spinous processes
- Heterotopic or dystrophic ossifications
In addition a bone scan is helpful in the investigation of back pain where other imaging is negative, does not correlate with the clinical findings, or has too many abnormalities. It casts a much wider net than either dedicated CT or MRI so has a role in defining poorly localised musculoskeletal pain.
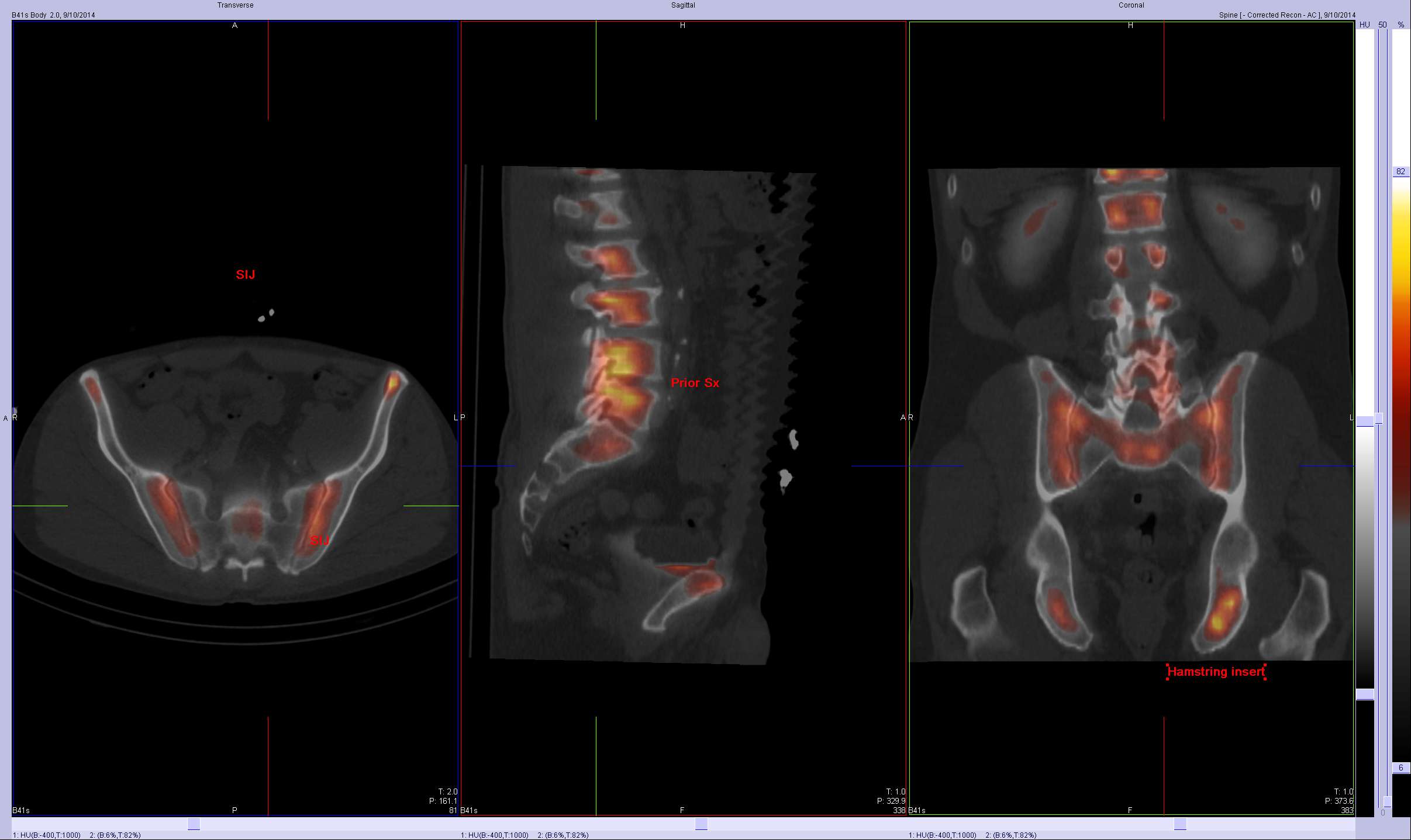
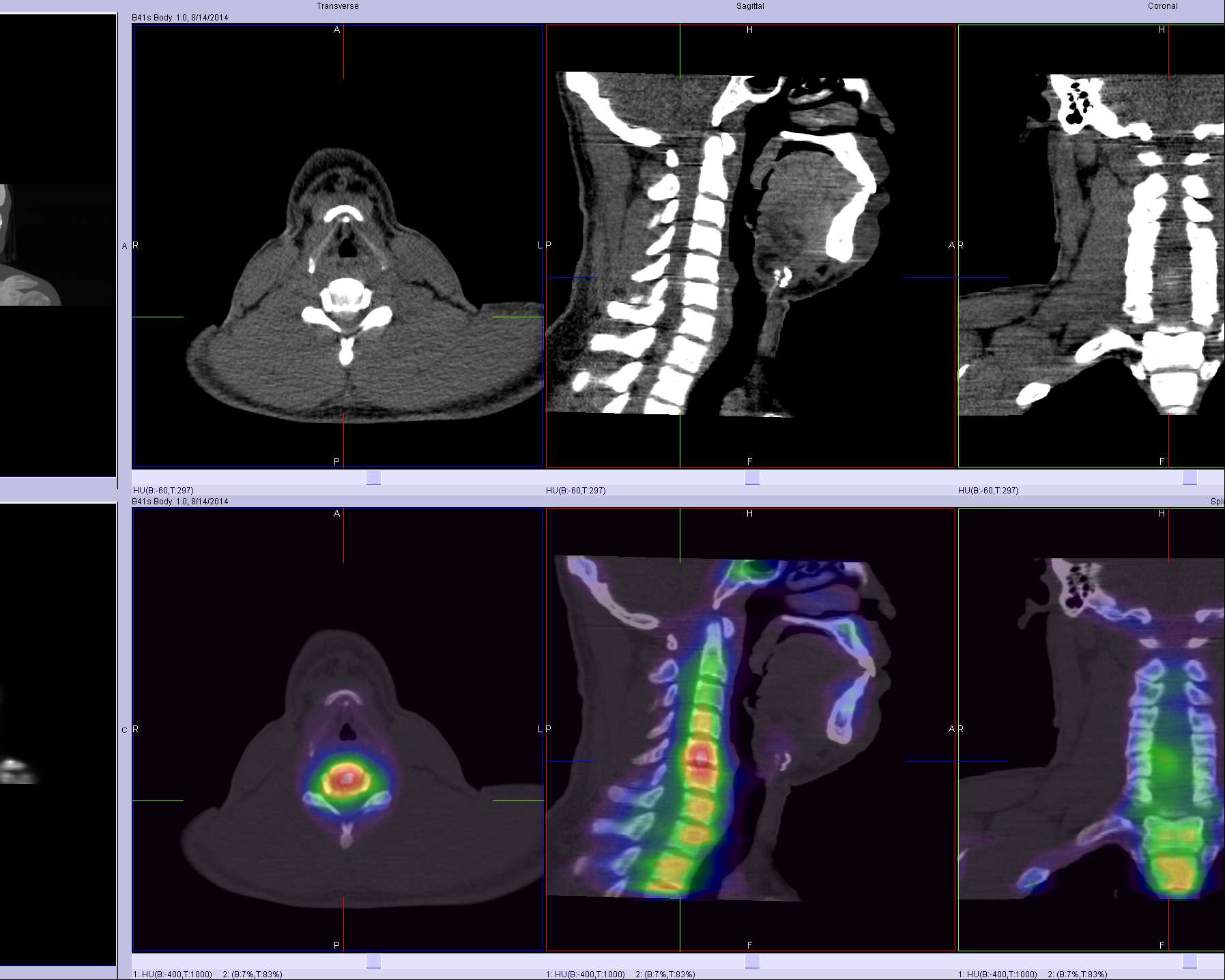
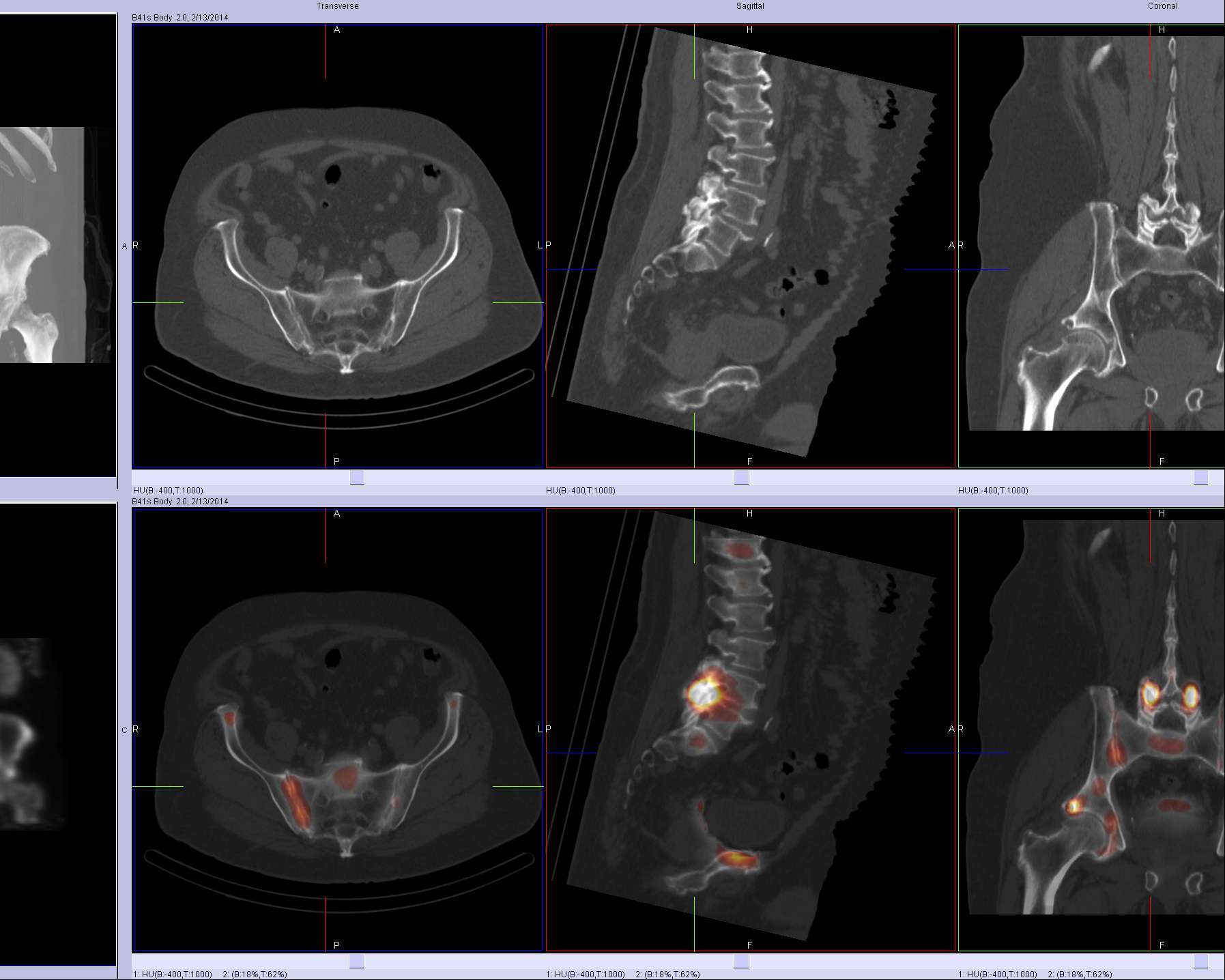
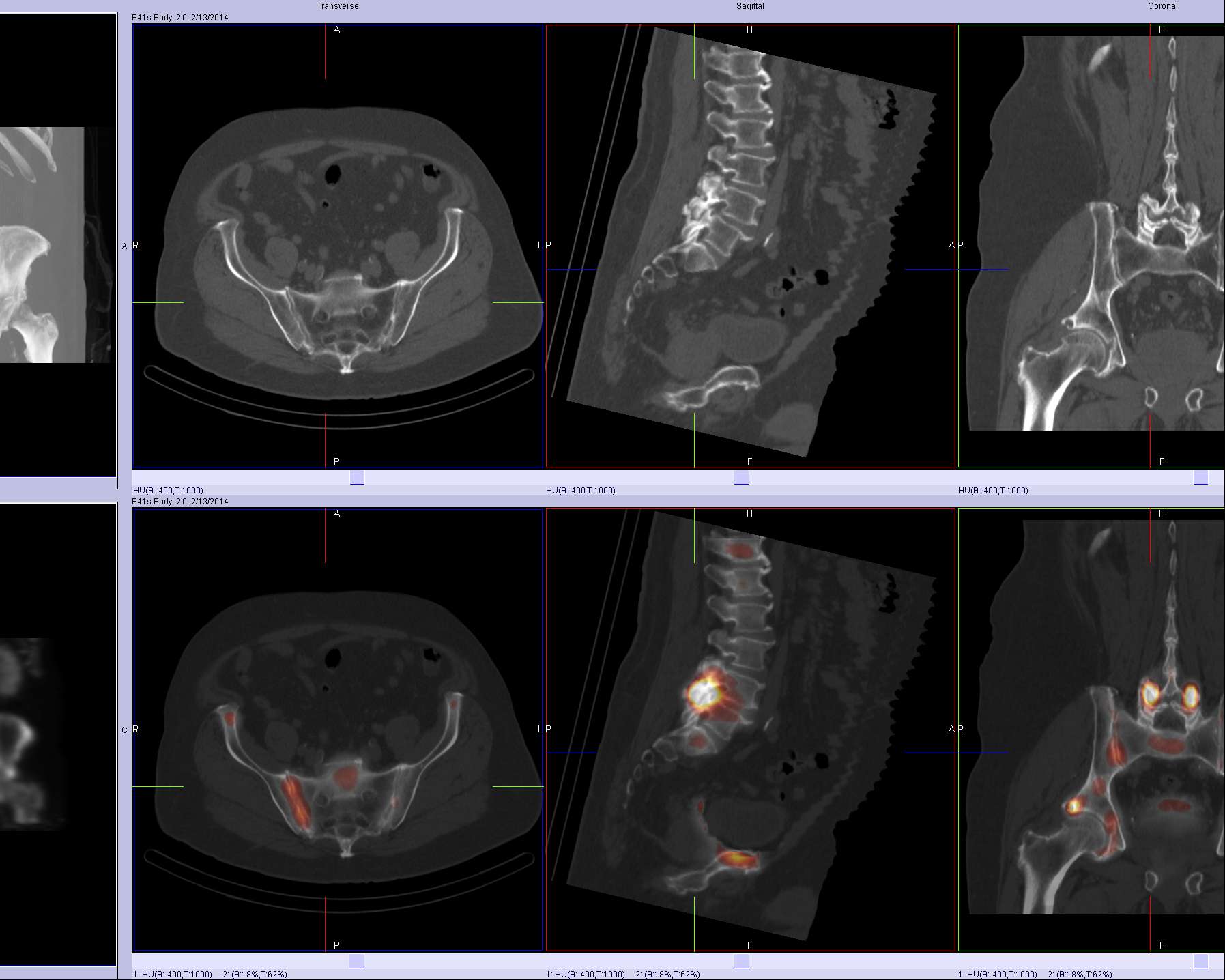
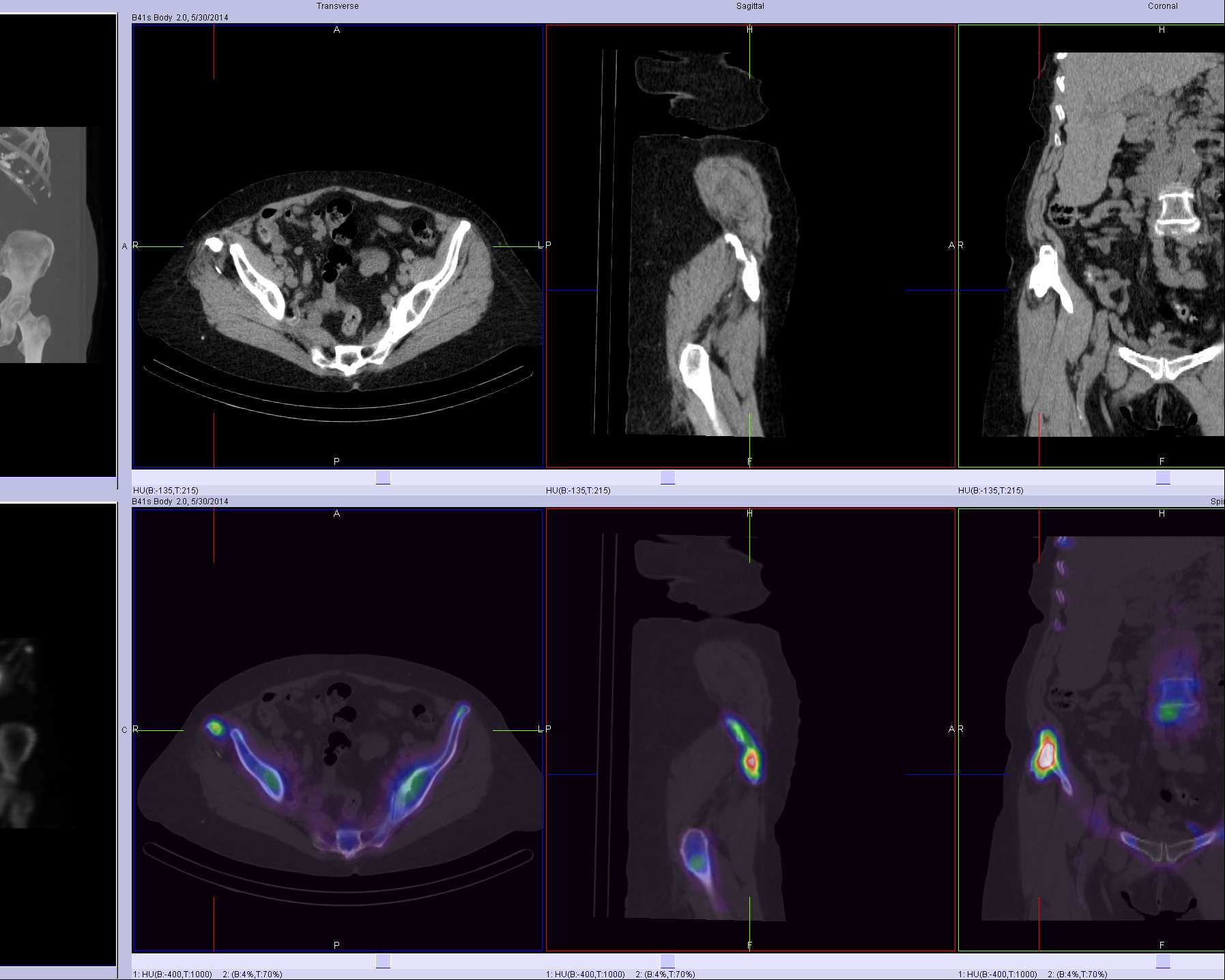
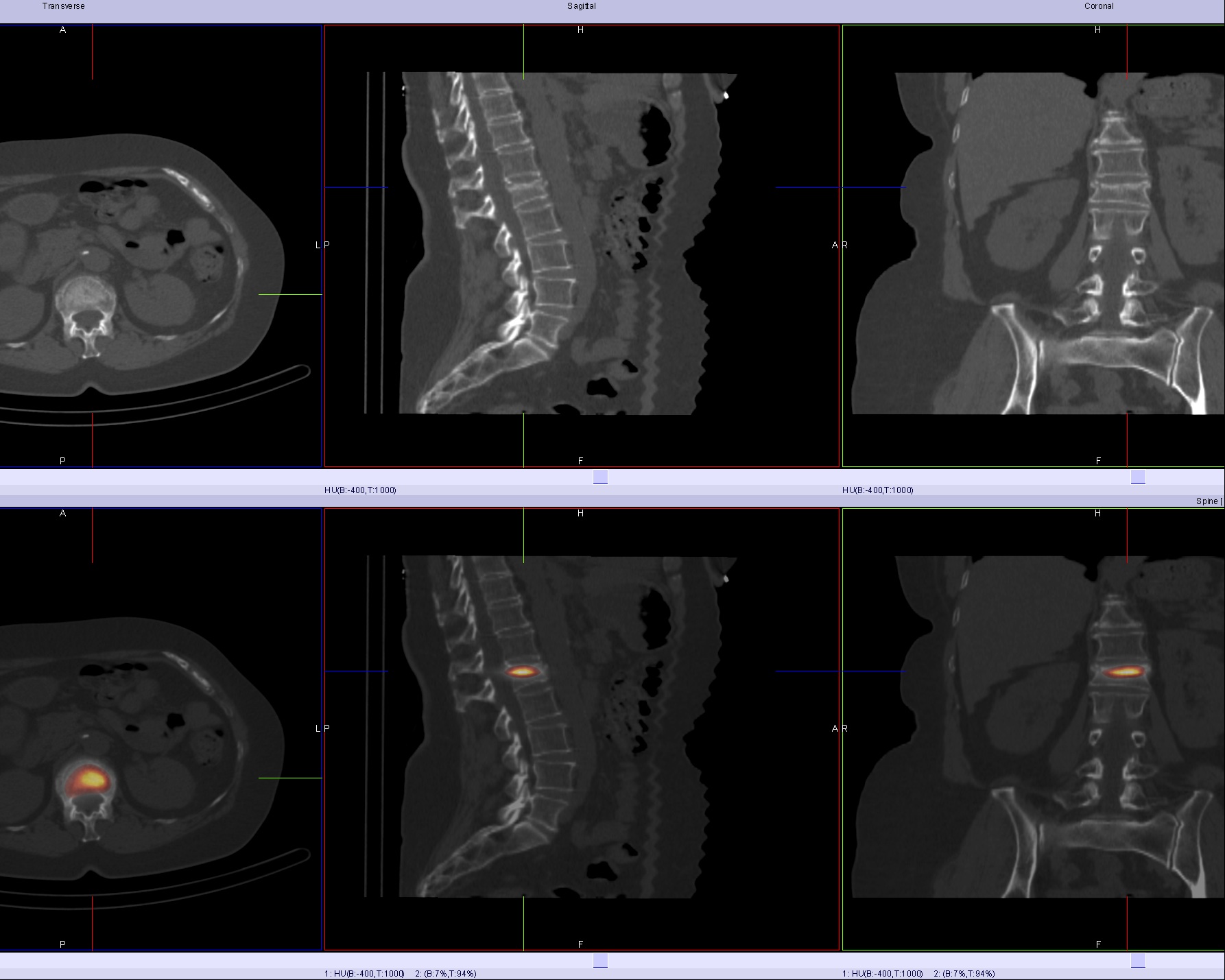
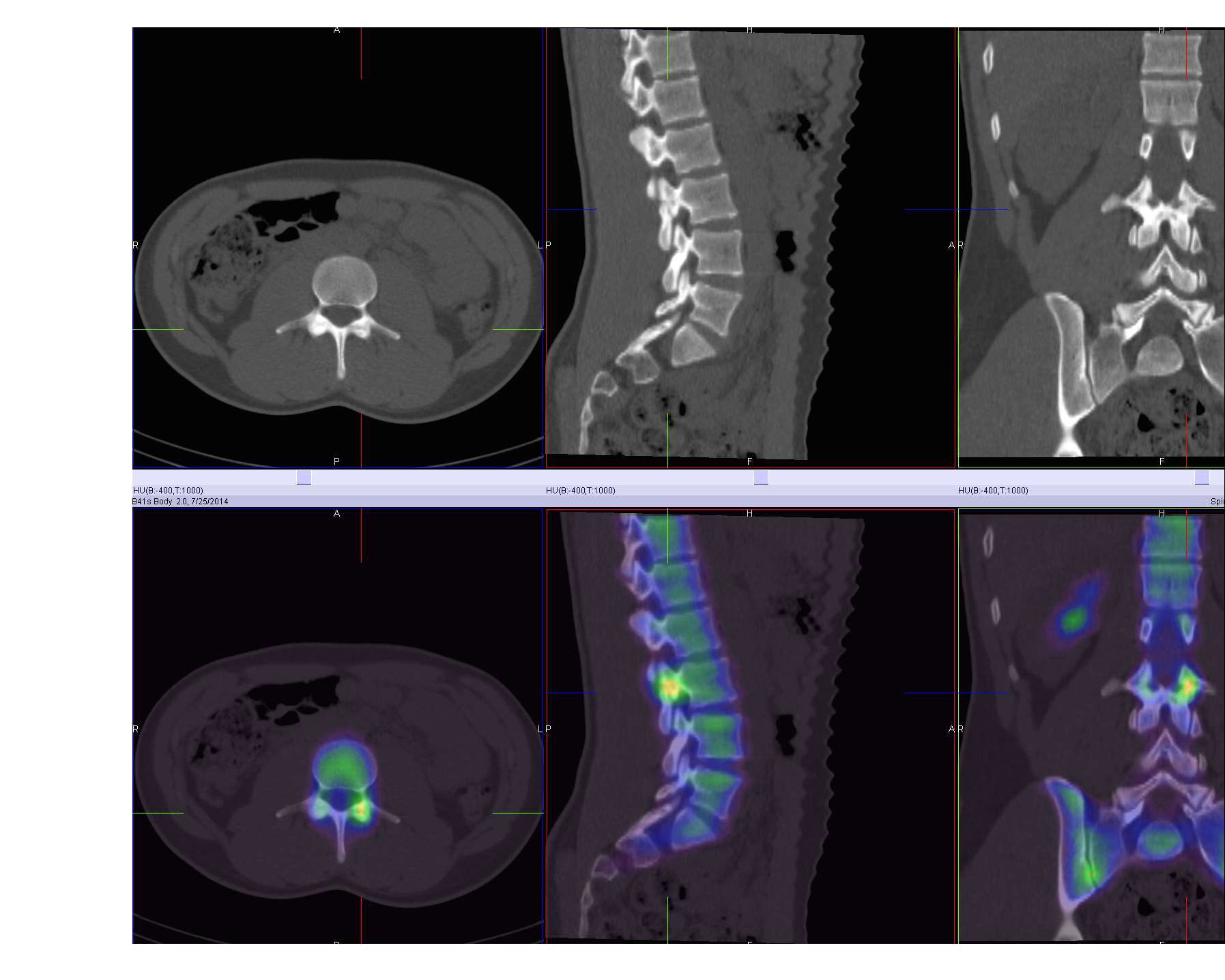
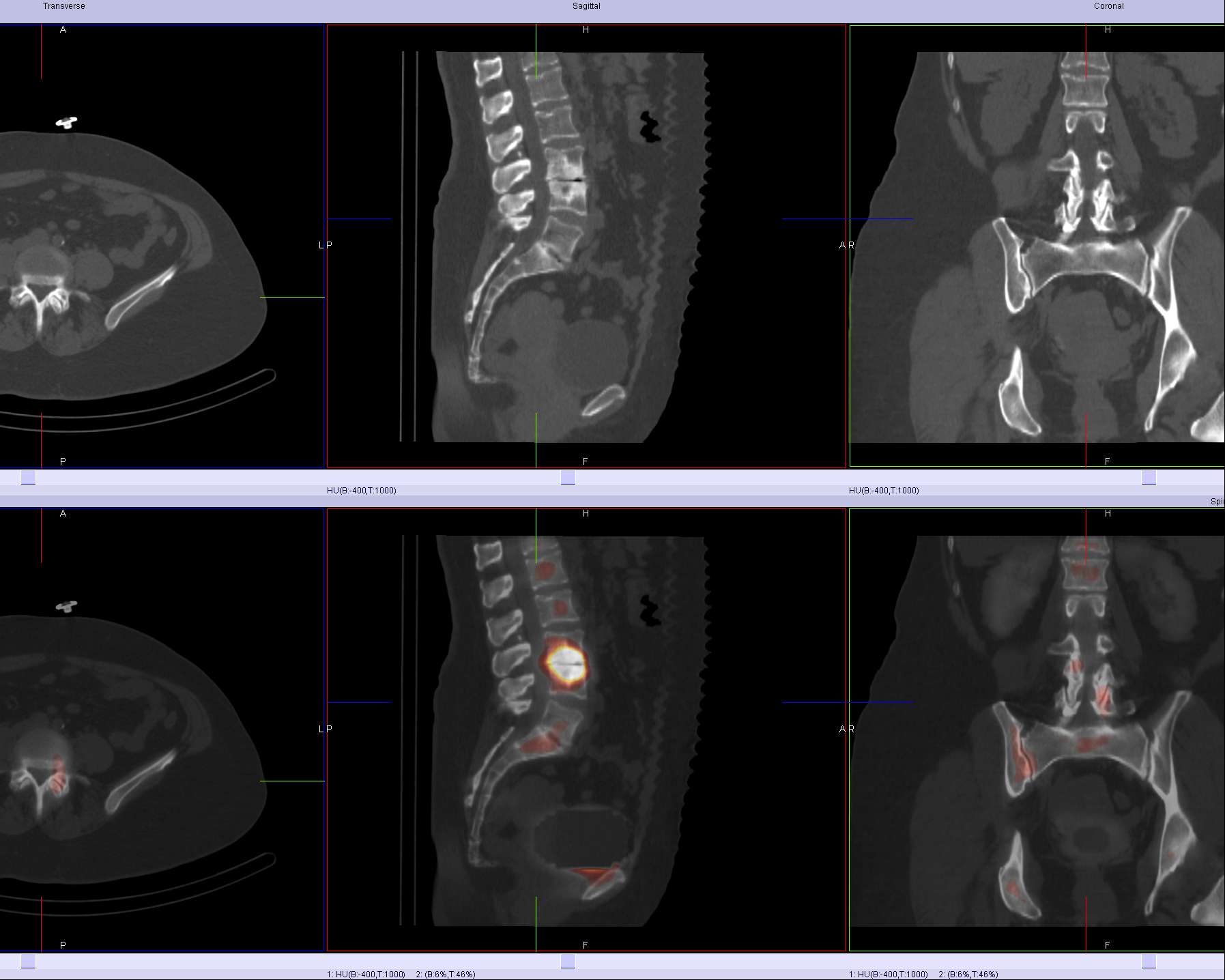
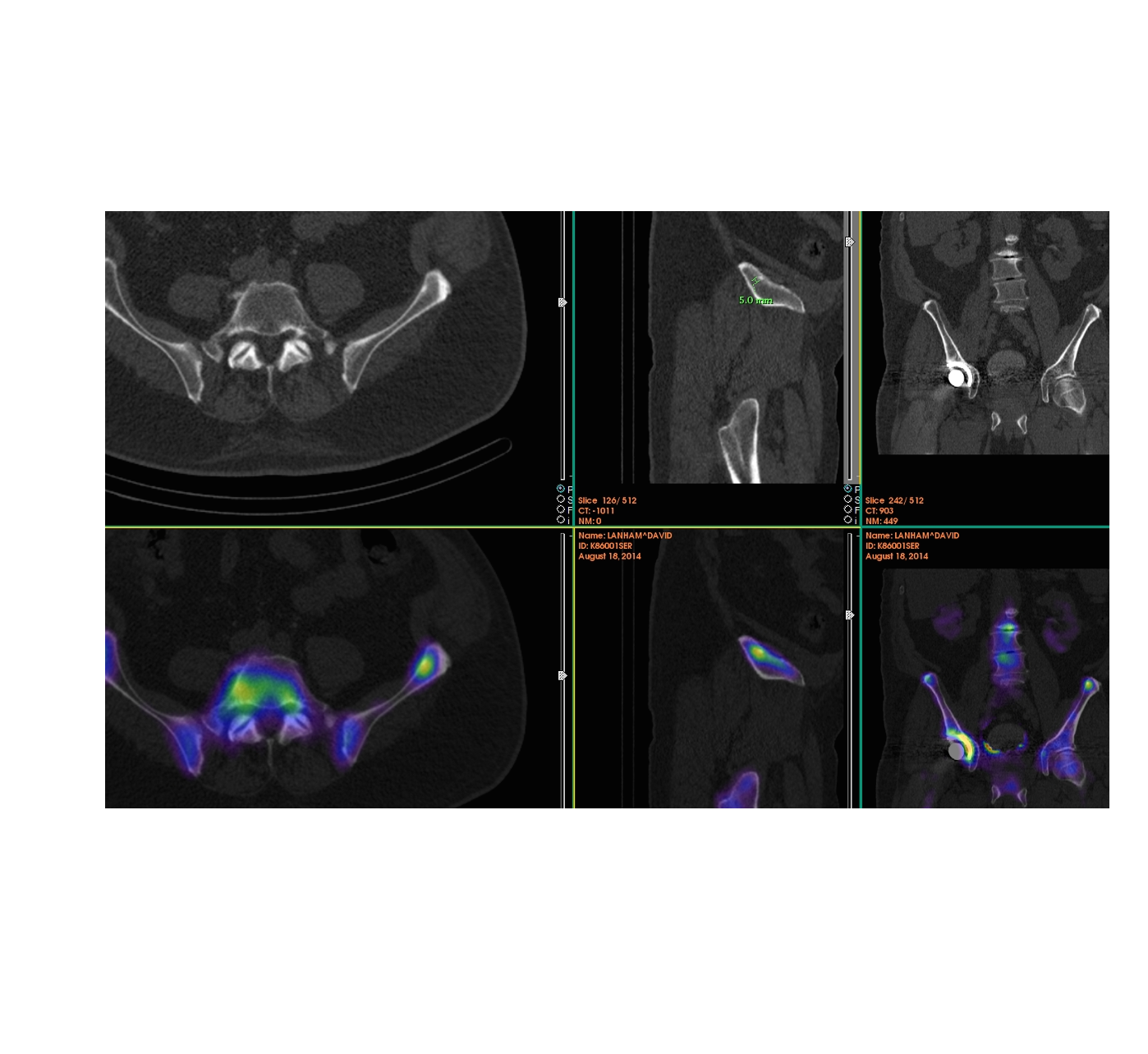
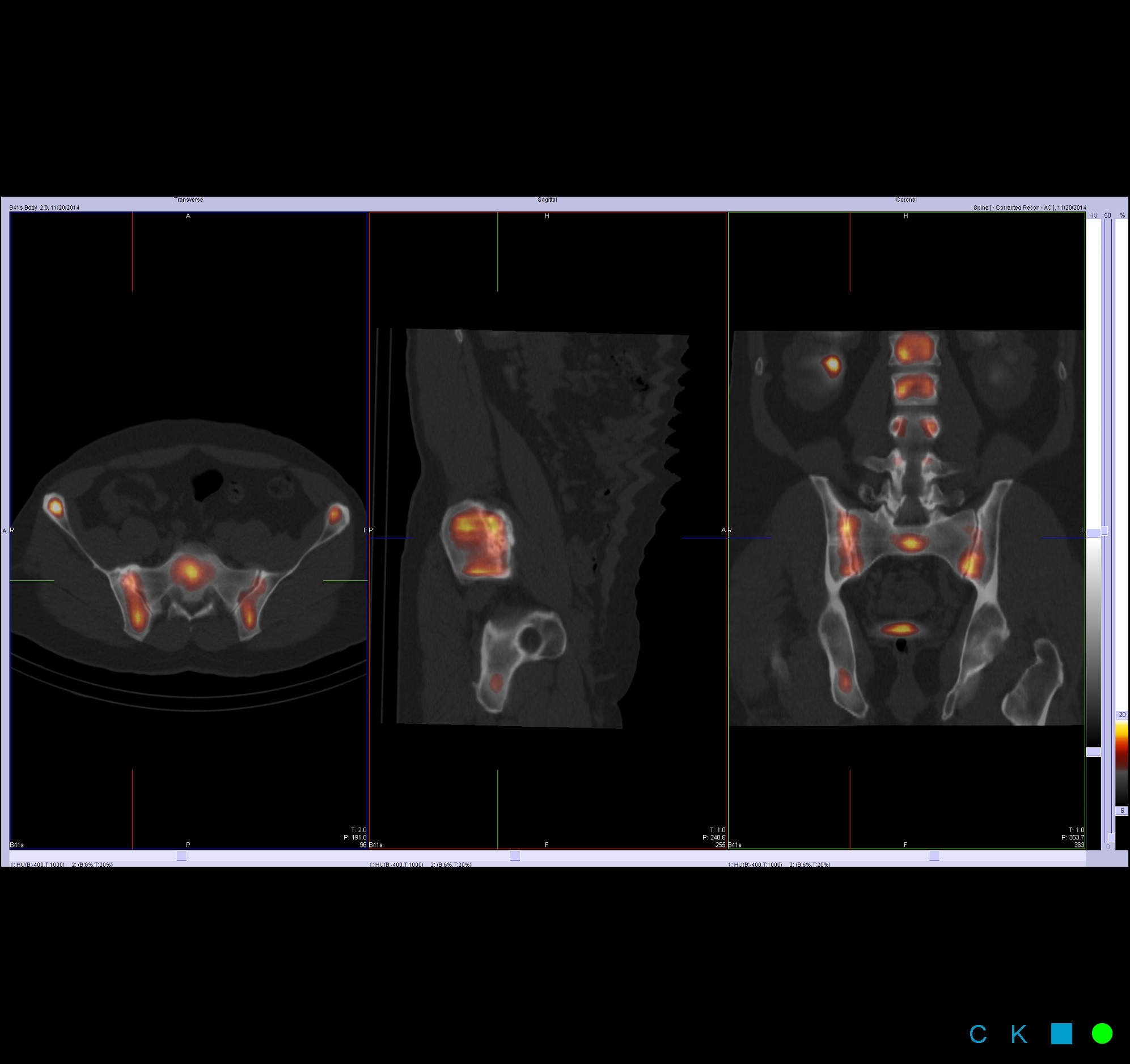
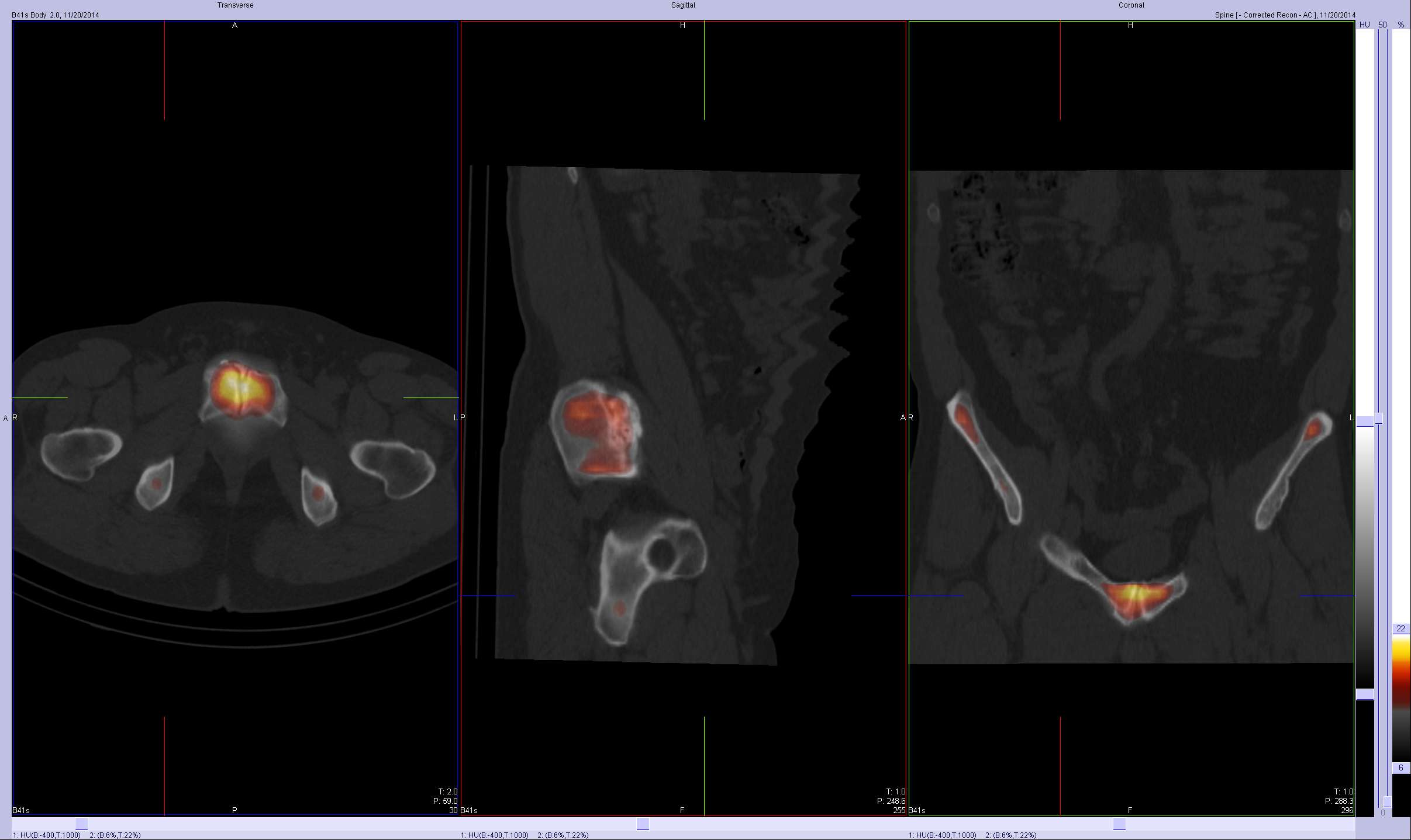
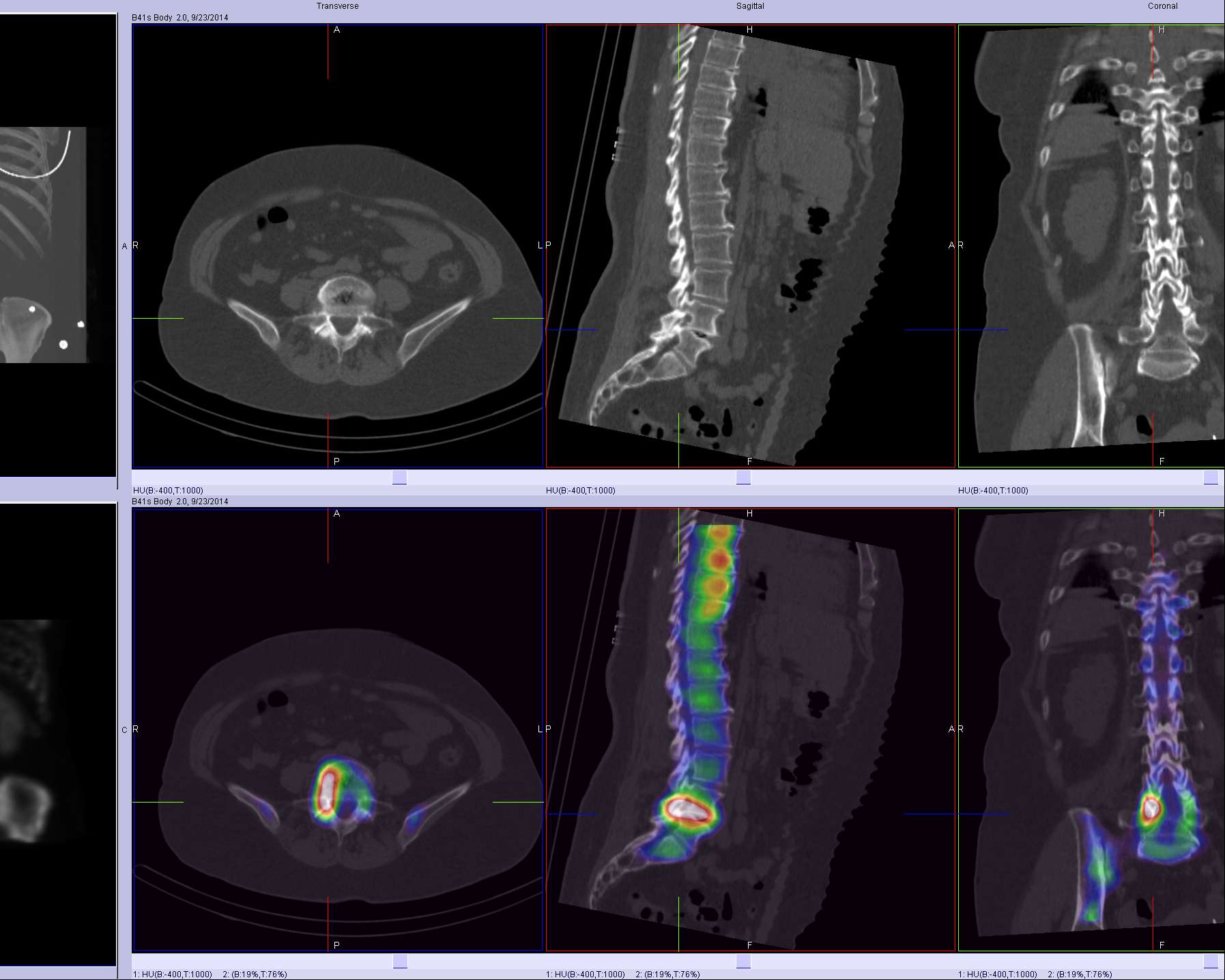
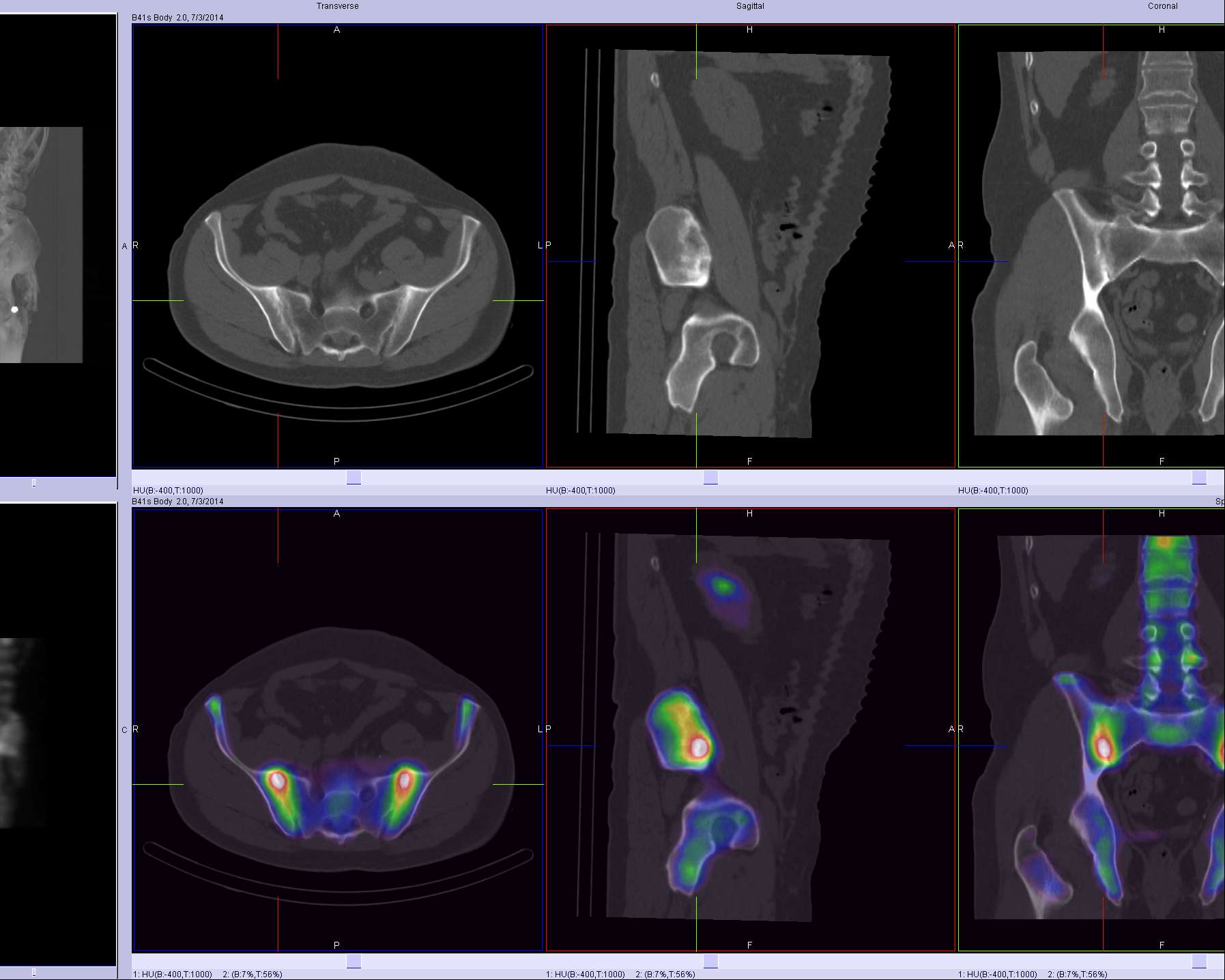
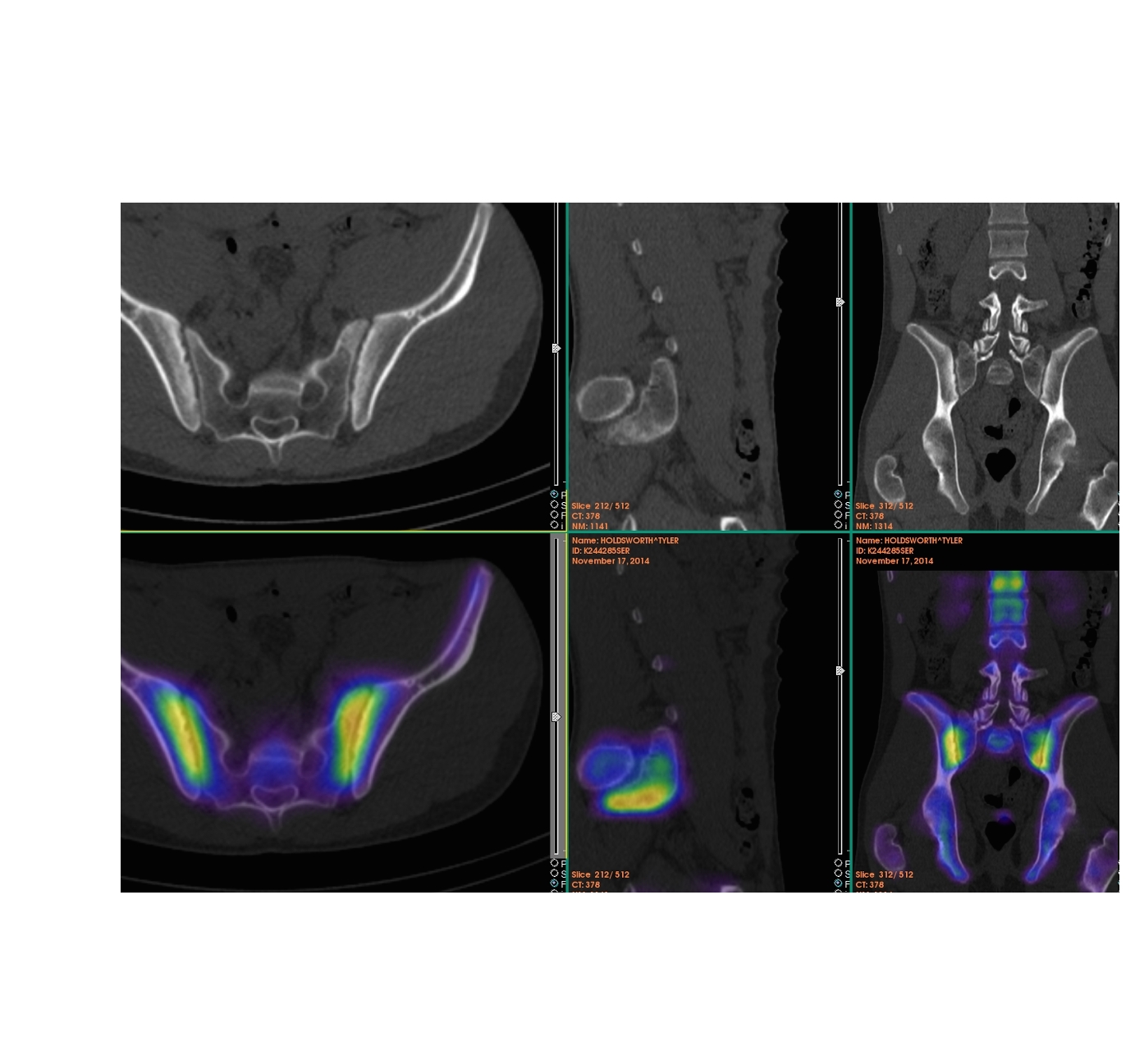
Some typical images:
References:
- Jain, A., Jain, S., Agarwal, A., Gambhir, S., Shamshery, C., & Agarwal, A. (2015). Evaluation of Efficacy of Bone Scan With SPECT/CT in the Management of Low Back Pain: A Study Supported by Differential Diagnostic Local Anesthetic Blocks. Clinical Journal of Pain, 31(12), 1054–1059. https://doi.org/10.1097/AJP.0000000000000212